
Healthcare Policy
The Role and Influence of Federally Established Health Policy Advisory Bodies in Canada
Abstract
Since the passage of the Canada Health Act (1985), there have been many advisory bodies established by successive federal governments, each tasked with providing advice and making recommendations about where and how to improve the health system. Our analysis of interviews with advisory board members and implementers (e.g., ministry of health leaders, staff and consultants) addresses why participants perceived their advice and recommendations were generally not implemented and informal strategy groups used to facilitate implementation. We recommend that future health system advisory bodies focus on coalition building during policy development, integrate implementation plans into policy recommendations and evaluate the impact of policy recommendations.
Introduction
As healthcare and the needs of Canadians have evolved, both federal and provincial/territorial governments have frequently established ad hoc health policy advisory bodies to guide health and healthcare decision making. Ad hoc advisory bodies, which are used across policy domains, use topical experts (Halffman and Hoppe 2005) and operate within the government sector, unlike policy institutes or think tanks (Lindquist 1993).
The use of royal commissions has been a popular policy tool in Canada and other commonwealth countries, particularly Australia (Mintrom et al. 2021); while presidential commissions have been used in the US (Zegart 2004). Commissions and other similar ad hoc advisory bodies can be conceptualized as primarily serving one of three core functions: (1) influencing the policy agenda; (2) providing evidence and information; or (3) building coalitions (Zegart 2004). Agenda commissions generate support for initiatives and target a mass audience; information commissions provide new facts and thinking about policies and target government officials; and coalition commissions seek to foster consensus among competing interests and coalition members (Zegart 2004). While commissions and similar advisory bodies are often viewed as deflecting blame from the government or giving the appearance that the government is taking action (Zegart 2004), many are intended to and succeed in shaping public policy (Mintrom et al. 2021; Zegart 2004). For example, the Royal Commission on Health Services led by Justice Emmet Hall was instrumental in the design and passage of key healthcare legislation, the Medical Care Act (1966), in Canada.
Since the passage of the Medical Care Act (1966) and the Canada Health Act (1985), there have been many federally established ad hoc healthcare policy advisory bodies that have addressed broad health system design challenges, including the National Forum on Health (1997), Romanow Commission (Commission on the Future of Health Care in Canada 2002), Kirby Committee (Standing Senate Committee on Social Affairs 2002), Advisory Panel on Healthcare Innovation (Advisory Panel on Healthcare Innovation 2015) and Advisory Council on the Implementation of National Pharmacare (2019). While each was national in scope, the Kirby Committee was established by the senate while the prime minister's office established the others. Despite the activities and their impact, there has been limited research on the role and influence of ad hoc advisory bodies in Canada. We aimed to understand the processes used to develop advice and recommendations as well as barriers, facilitators and outcomes of the implementation of advice and recommendations.
Methods
Conceptual framework
The conceptual framework guiding this study is based on Bullock et al.'s (2021) recent synthesis of policy implementation literature and implementation science literature. Our conceptual framework (Figure 1) integrates two parts of a policy implementation framework, namely, the policy process and determinants, developed by Bullock et al. (2021).
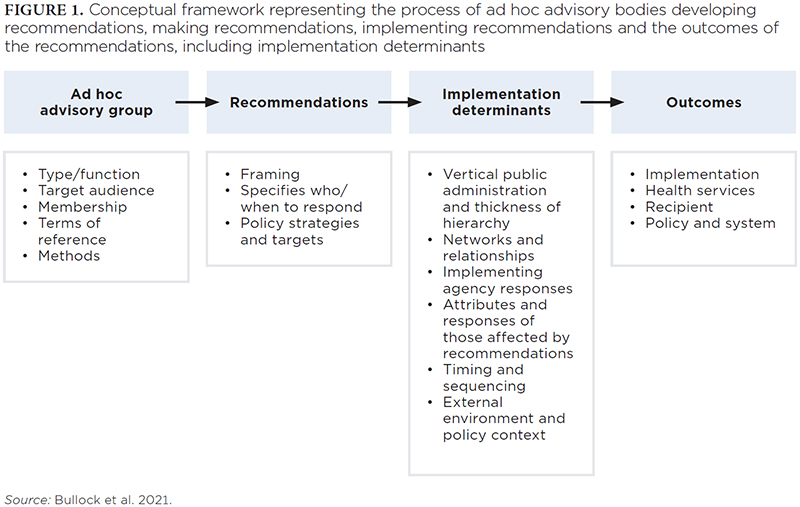
The implementation process framework includes the advisory body's policy development process, the policy package (i.e., the group's recommendations), active implementation and outcomes. The advisory body's policy development process would be influenced by the external context as well as their internal context, including intended and unintended functions of the group, group members and methods. The recommendations themselves could be influential based on how they were written; what types of policy strategies and targets were included; number and specificity. The implementation of recommendations could be influenced by the characteristics of recommendations and group processes as well as identified determinants of implementation, such as timing and sequencing, external environment/policy context, use of top-down or bottom-up approaches and relationships and responses of policy actors. In the healthcare sector, in particular, the attributes and responses of those affected by recommendations are critical implementation determinants due to the joint jurisdiction of healthcare. A range of outcomes are possible, including implementation of recommendations; impact on Canadians; and impact on health policy, healthcare services and the health system.
Participant selection and recruitment
We identified advisory body members and implementers through reports prepared by each advisory body, including the National Forum on Health (1997), Romanow Commission (Commission on the Future of Health Care in Canada 2002), Kirby Committee (Standing Senate Committee on Social Affairs 2002), Advisory Panel on Healthcare Innovation (2015) and Advisory Council on the Implementation of National Pharmacare (2019). We included these advisory bodies because they were ad hoc groups with a mandate from the federal government to provide advice and make recommendations about structural health and healthcare system policies, predominately related to healthcare funding, coverage and delivery, after the passage of the Canada Health Act (1985). We excluded inquiry-focused advisory bodies that addressed a specific health issue, such as the Krever Inquiry and the National Advisory Committee on SARS and Public Health.
After we created a sample frame of advisory body members and implementers (e.g., ministers of health when reports were released, the federal government staff who supported the advisory bodies), we recruited participants using a combination of purposive and snowball sampling. We aimed to recruit at least one advisory body member and one implementer from each advisory body for a total of at least 10 interviews. We initially contacted advisory body members and implementors in leadership positions in the advisory body or government of the time using publicly identified e-mail addresses. When unsuccessful, we reached out to the other advisory group members or attempted other communication strategies, such as LinkedIn messages. Furthermore, at the end of each interview, we asked the participants whom they would recommend we interview. Recruitment and data collection took place from May to October 2022.
In-depth interviews
We conducted interviews with participants over Zoom. Interviews ranged in length from 50 to 90 minutes. An interview protocol based on our conceptual framework was used to guide the interviews (Appendix 1, available online here). Interviews addressed the advisory body's mandate and processes (e.g., how the group worked together and with the government and what methods they used to solicit information from experts and citizens) as well as the implementation and impact of the advisory body's recommendations, including what the participant considered the greatest success of their report and what the barriers and facilitators were of implementing the report's recommendations. Interview proceedings were audio recorded, transcribed, deidentified and imported into NVivo 12 software (Lumivero 2017).
Analysis
Two authors (Amity E. Quinn [AEQ] and Rachelle Drummond [RD]) conducted a reflexive thematic analysis (Braun and Clarke 2006, 2019; Byrne 2022). Reflexive thematic analysis is a theoretically flexible type of thematic analysis to identify patterns of meaning that are not concerned with coding reliability or structured codebooks. It involves a process of data familiarization, data coding and theme development and revision. Themes, created from both codes and researchers' active engagement with data, are the output of the analysis.
AEQ and RD each participated in the interviews and independently reviewed the transcripts. They discussed the initial codes and agreed upon a first draft codebook based on our conceptual framework. After coding the first four transcripts, AEQ and RD refined the codebook. RD then independently coded the subsequent transcripts. Initial coding was predominantly deductive, following the conceptual framework. RD summarized the results within each code and subcodes. AEQ and RD engaged in a series of conversations to discuss the coding and to develop themes using an inductive process. These discussions led to substantial consolidation of themes through the consideration of both authors' interpretations of the data until themes were finalized.
This study was approved by the University of Calgary Conjoint Health Research Ethics Board (REB22-0156).
Results
We invited 22 individuals to participate. Twelve agreed to participate, one declined and the others did not respond to initial and follow-up messages. Of the 12 participants, nine were members of advisory bodies and three were implementers. Advisory body members included physicians, professors, policy experts and politicians. Implementers included political and civil service leadership and consultants to the federal ministry of health. Three of the participants were women, and nine participants were men. Because two of the implementers were involved in multiple reports, there were at least two interviews that addressed each of the five advisory groups of interest, which included the National Forum on Health (1997), Romanow Commission (Commission on the Future of Health Care in Canada 2002), Kirby Committee (Standing Senate Committee on Social Affairs 2002), Advisory Panel on Healthcare Innovation (2015) and Advisory Council on the Implementation of National Pharmacare (2019).
We identified three themes: (1) individuals have different interpretations of the policy impact of their recommendations; (2) conflict between different levels of government was a major implementation barrier; and (3) informal implementation strategies can facilitate implementation at different levels of government.
Individuals have different interpretations of the policy impact of their recommendations
Participants had different interpretations of the success or failure of their advice and recommendations. Most participants perceived a lack of implementation of their recommendations as a failure (based on personal interpretation) and were disappointed with how little concrete federal health policy change there has been in Canada since the 1990s.
Some participants did view the creation of the advisory bodies and their reports as a success. For example, even when most of their recommendations had not been implemented, these reports “shaped the [health policy] discussion for a generation” (P3, Advisory Body Member). The concept of the report as an influential idea was also articulated by a participant:
One of the things I learned with public policy is that sometimes it can take a long time before anything gets adopted. I always look at public policy as what the idea is. It's kind of like a dripping. When a report comes out, there's an idea there. It takes many, many years, and then all of a sudden, swoosh, something gets adopted (P6, Advisory Body Member).
Participants highlighted that resistance to change remained despite the formation of the advisory body by the government, extensive research directed or solicited by the advisory body and extensive consultation with various levels of government and Canadians. One participant involved in the Romanow Commission expressed their frustration with the failure of implementation and lack of change:
You look at the [National Forum on Health] table of contents and those are all the issues that we grappled during the Romanow Commission. There's some of the same issues we're grappling with in 2022. So, there is that level of frustration that we did all that work and commissioned all of that research to make the case and so little of it got taken up (P10, Advisory Body Member).
Furthermore, participants noted that many recommendations have been repeated in multiple reports, yet never implemented. Thus, when implementation does take place, it is difficult to attribute one advisory body as responsible for the success. Moreover, some participants reported that implementation was not part of the mandate or welcomed. And, in one case, the advisory body was terminated early and before implementation was considered.
Some participants, however, viewed the lack of implementation of repetitive recommendations as a necessary component of subsequent implementation. These participants noted that policy change can require a continuous push from experts and citizens over time. This perspective was reflected in the following statement:
When you look at some of these reports, we get frustrated that this has been said three times, but in truth, if it wasn't said three times, the fourth one wouldn't have the frustration of saying, “Enough is enough” (P9, Advisory Body Member).
In addition, some participants thought that repetitive recommendations provided insight into what Canadians or Canadian institutions want and, thus, influenced the political agenda. As one participant said:
It is interesting that the policy reforms advocated for in that report are the same that have been reinforced for the last 10 years, but it also is reflective of what Health Canada is interested in (P12, Implementer).
Conflict between different levels of government was a major implementation barrier
Prominent ongoing conflict was identified by all participants as one of the largest barriers to implementation. Participants discussed three distinct categories of conflict: (1) between provincial/territorial governments and the federal government; (2) within the federal government; and (3) between Canadians and the federal government.
Conflict between provincial/territorial governments and the federal government was the most frequently discussed type of conflict. Participants described this conflict as primarily stemming from the long-standing mistrust between the two levels of government arising from the division of power in the Constitution Act (1867) or resulting from cutbacks to federal healthcare spending contributions, such as those seen in the 1994–95 federal budget, which one participant referred to as a “bomb” (P10, Advisory Body Member).
Participants discussed that even when the federal government may want to move forward with the implementation of advisory body recommendations, the shared jurisdiction of healthcare relies on cooperation from provincial/territorial governments. One participant discussed that the lack of cooperation between provinces/territories and the federal government on healthcare reform is due to political differences. For example, when speaking about pharmacare, this participant explained:
I think that Health Canada would probably like to make progress on pharmacare, but there are a number of provinces that don't want any part of it … the political ideologies of the different provinces … that are not aligned with the federal government pose these really tricky problems (P12, Implementer).
Conflict within the federal government was the second most frequently discussed type of conflict. At this level, participants identified conflict within advisory bodies themselves (e.g., priority disagreements) as well as between the advisory body and ministries and between ministries themselves, particularly health and finance. Changes in ministry leadership had the potential to substantially impact the advisory body's process. For example, during the National Forum on Health, the change of health minister led to the reduction of the group's budget, timeline and potential for implementation and distribution of their report. Similarly, initiatives championed by the ministry of health without support from the ministry of finance (indicated by allocated funds in a budget) or the prime minister's office, such as the Advisory Panel on Healthcare Innovation, are unlikely to be implemented. For example:
I also met the health minister of the day … And she also seemed very interested and engaged in the process. The only thing that would seep out from time to time was, although she was very engaged, it really wasn't clear that the conservative cabinet was very engaged. So there was sort of a feeling that she was a bit of an outlier, or it was kind of a personal mission rather than it was supported by the government of the day. So, that was a bit concerning (P7, Advisory Body Member).
Conflict between the federal government and Canadians was the least frequently discussed type of conflict. Participants emphasized the importance of minimizing this type of conflict to generate citizens' support for healthcare reform. This type of conflict could arise from citizens' seemingly contradictory perspectives that the federal government did not follow through on promises of change and that change could threaten the current healthcare system, of which Canadians are very protective. As one participant explained:
I think the protection of the status quo as it exists is more damaging and actually will unravel the system. Our biggest enemy are those that are protecting the status quo (P3 Advisory Body Member).
Informal implementation strategies can facilitate implementation at different levels of government
As several participants discussed, advisory body members were typically not legally permitted or welcomed to have an explicit role in implementing their proposed recommendations. These ad hoc federal advisory bodies dissolved following the submission of a report. Despite having no explicit role, participants shared a range of informal strategies they used within the federal government, with provinces/territories and with the public both during and after the development of their recommendations to facilitate implementation.
Implementation strategies at the federal government level included the prime minister chairing the advisory body (e.g., National Forum on Health), recurring meetings with the minister of finance and the ministry of health or parliamentary staff serving on the advisory body. Bureaucratic staff serving in the advisory body had the role of “le fonctionnaire” (P1, Implementer), which provided a bridge between the group's recommendations and the government's reassessment of the recommendations and potential implementation. Implementation strategies at this level also included activities within and between advisory bodies, such as (1) meetings between members of the National Forum on Health and the Romanow Commission and (2) the Romanow Commission's very detailed recommendations that included timelines and designated responsibility, which participants explained were intentional because advisory body members had worked in government and were aware of the governmental process to implement policy recommendations.
Efforts to engage provinces and territories to foster implementation while developing their recommendations included consultation and coalition building, such as travelling to each province or territory for meetings. The Romanow Commission included an intergovernmental affairs officer on its small staff specifically for this purpose. A couple of participants discussed how advisory body members with personal relationships with provincial/territorial governments continued to meet informally with provinces and territories after the report was released.
All participants noted the public as invaluable to the implementation process, both during and after the development of the report. Efforts to engage Canadians while writing the report included gatherings and presentations, often in the form of town halls. Following the publication of their reports, several former advisory board members took it upon themselves to further disseminate the report to the public through presentations, media and follow-up reports.
| TABLE 1. Summary of implementation barriers and facilitators across different levels of government | ||
| Implementation barriers | Level of government | Implementation facilitators |
| Lack of alignment between the advisory body, prime minister, ministry of health and ministry of finance | Within the federal government* | Group membership Recurring meetings with the minister of finance Meetings between members of different advisory bodies Detailed recommendations, including timelines and designated implementers |
| Shared jurisdiction of healthcare High level of mistrust due to continued reductions in federal healthcare spending contributions Political differences | Federal government* and provincial/territorial governments | Consultation Coalition building Intergovernmental staff role Members continued meetings with personal connections in provinces and territories after advisory bodies dissolved |
| Perception that federal government did not follow through on promises of change Perception that change could threaten the current healthcare system Symbolism of medicare | Federal government* and citizens | Engagement in the development of recommendations (e.g., townhalls and focus groups) Presentations, media and publications following the report |
| *Because advisory bodies are considered part of the federal government, this includes actions the advisory body themselves undertook during or after the development of the recommendations as well as advisory body actions related to the broader federal government's relationships. | ||
Discussion
Based on interviews with members and implementers of federally established advisory bodies on health system design since 1990, we identified three themes: (1) individuals have different interpretations of the policy impact of their recommendations; (2) conflict between different levels of government was a major implementation barrier; and (3) informal implementation strategies can facilitate implementation at different levels of government.
Participants perceived that the federal government generally did not implement the recommendations of ad hoc health system-focused advisory bodies. As such, our detailed conceptual framework ultimately was not useful because there was too little implementation of the advisory body's recommendations to allow us to probe into implementation processes, determinants and outcomes. Matland's (1995) ambiguity-conflict model of policy implementation provides a more useful lens to understanding advisory body function and actions, the lack of implementation of recommendations and strategies to promote change. Matland's (1995) model describes the implementation processes along two axes: ambiguity and conflict. Ambiguity can exist around policy goals as well as policy means (e.g., external context, policy actor roles in implementation). Conflict occurs when there is interdependence between actors and is often evoked by symbolic policies. In areas with high ambiguity and high conflict, defining successful implementation is difficult and implementation is less likely. Furthermore, when implementing policy in areas of high ambiguity and high conflict, the role of policy actors with professional training – such as advisory body members – and the role of coalitions are essential (Matland 1995).
As is clear from our results and current news, health system reform in Canada is an area with high ambiguity and high conflict. Health policy is complex and highly symbolic, and there is interdependence between federal and provincial/territorial governments with a lack of clarity around specific implementation roles and responsibilities. Advisory bodies are composed of public members as well as professionals and experts with a range of relevant training and are able to navigate ambiguous policy goals and means as well as conflict between policy actors. To do this, the advisory bodies that we studied appeared to play multiple functions, including agenda setting, information gathering and coalition building (Zegart 2004) in an effort to reduce ambiguity and conflict, including their engagement with experts as well as the federal government, provinces/territories and citizens and creation of specific staff roles such as an intergovernmental affairs officer. Nevertheless, the policy advice and recommendations that they proposed ended up being successful as ideas for health policy experts or future policies.
Based on our findings, we propose three strategies for policy advisors to consider to improve the outcomes of future health system advisory bodies: (1) prioritize coalition building; (2) integrate implementation plans; and (3) require evaluations of advisory body reports and processes. These strategies are supported by findings on the influence of royal commissions in Australia, which found successful reports from royal commissions included coalition building, particularly listening to people and recognizing the power of emotion holding coalitions together, detailed implementation plans and required monitoring and reporting on the implementation process (Mintrom et al. 2021). Moreover, these strategies could be used by individual health policy experts when advising decision makers.
1. Prioritize coalition building
Conflict at different levels was the major barrier to the implementation of advisory bodies' recommendations. Advisory bodies were not only aware of that but also attempted numerous strategies to build coalitions in order to overcome the conflict, such as citizen engagement (McIntosh and Forest 2010). Because conflict will likely remain an issue in national health policy considering the joint provincial and federal jurisdiction, coalition building could facilitate the implementation of future advisory group recommendations.
There are several advantages of coalitions, specifically in the health context, including involvement without direct responsibility for the solution, demonstration of public support for an issue and maximization of power of each member as they come together through joint action (Butterfoss et al. 1996). Together, these advantages can promote policy implementation through goal alignment (Butterfoss et al. 1996). Strategies used by advisory groups in this study to engage both citizens and private industry in coalitions include engagement in the development of recommendations (e.g., town halls and focus groups) and presentations, media and publications following the report. Coalition members could also be integrated into implementation and evaluation plans.
2. Integrate implementation plans
Advisory body members do not have an explicit role in the implementation process. Final reports typically had no or few stated implementation plans, which relates to the interview findings regarding the lack of government mandate to implement advice and recommendations. In contrast, the Romanow Commission – which is arguably the most successful advisory body we studied because of the subsequent passage of the 2004 Health Accords (Health Ministers of Canada 2004) – intentionally included implementation details, such as timelines and responsible parties. Implementation plans that identify timelines, goals and clearly defined roles and responsibilities can reduce ambiguity to facilitate the implementation of the recommendations.
Implementation plans can be informed by political science, implementation science or policy implementation science literature. Bullock et al. (2021) provide suggestions for implementation strategies based on policy targets and strategies. Creating dedicated funding sources that align with the time required for implementation is an example of an implementation strategy for system-level policy change that targets financial arrangements. From the implementation science literature, the Long Term Success Tool (Lennox et al. 2017) or the Intervention Scalability Assessment Tool (Milat et al. 2020) can inform health policy implementation plans, including an assessment of acceptability, setting and workforce; implementation infrastructure; and sustainability.
3. Require evaluations of advisory body reports and processes
Evaluations of the advisory bodies that we studied were not required. Our interviews regarding the success or failure of the implementation of recommendations often seemed to be the first assessment of the report, coming decades after most of the groups we studied. More recent ad hoc federal advisory bodies have been required to conduct evaluations, including the Task Force on Cannabis Legalization and Regulation (2016). Evaluations have the potential to facilitate implementation by creating an accountability mechanism while allowing for an assessment of the implementation process and outcomes. Furthermore, evaluations of advisory bodies can improve our understanding of their purpose and the role that they play in policy implementation.
A range of evaluation approaches could be considered. A 2017 Royal Commission in Australia recommended strategies to monitor the implementation of their report, which could be adapted as follows (Mintrom et al. 2021): First, national, provincial and territorial governments could be required to indicate if they accepted, rejected or wanted further discussion with respect to an advisory body's recommendations. Second, the federal government could publish annual reports on implementation progress for a certain number of years immediately following the advisory body activity. Third, other institutions or groups (e.g., coalition members or advisory body members) could also make annual reports on implementation progress. Last, a review of the implementation could be conducted after approximately 10 years of the advisory body report.
There are several limitations to this study, particularly around the understanding of the advisory bodies themselves and our analytic approach. First, the intention of a specific advisory body is challenging to determine. While we did ask participants about the intention behind their advisory group, there was a range of perspectives among participants if their recommendations were expected to be adopted, either when the group was formed or during the process. Conducting interviews or using other evaluation methods closer to the advisory body's activity could provide a clearer understanding of the advisory group's intention and impact. Second, in focusing on the implementation of the advisory body's recommendations, we assumed that the recommendations of the advisory body were reasonable. It was beyond the scope of this paper to evaluate the appropriateness of the recommendations themselves. Third, we did not beta-test the interview guide. However, the interview guide was designed to be semistructured and refined before and during data collection to reflect suggestions from our research team and our experience in initial interviews (Appendix 1, available online here). Last, we conducted 10 interviews about five advisory bodies and did not attempt to achieve saturation (of data or meaning). While the number of interviews and absence of saturation may impact the external validity of our findings, our approach to data collection and analysis (reflexive thematic analysis) was selected intentionally to acknowledge the subjectivity of advisory group members' and researchers’ perspectives.
Conclusion
Participants perceived that the federal government generally did not implement the recommendations of ad hoc health system-focused advisory bodies. Despite the implementation strategies that groups used to engage federal ministries, provincial/territorial governments and citizens, the persistent conflict surrounding the highly symbolic policy of medicare ultimately resulted in a symbolic implementation of the reports as influential ideas for health policy experts or future policies. To improve the outcomes of future health system advisory bodies or other policy development processes, policy advisors should prioritize coalition building during policy development, integrate implementation plans into policy recommendations and evaluate the impact of the policy recommendations.
Correspondence may be directed to Amity E. Quinn by e-mail at amity.quinn@ucalgary.ca.
Rôle et influence des organismes consultatifs en matière de politiques de santé établis par le gouvernement fédéral au Canada
Résumé
Depuis l'adoption de la Loi canadienne sur la santé (1985), de nombreux organismes consultatifs ont été créés par les gouvernements fédéraux successifs et chacun d'entre eux est chargé de fournir des conseils et de formuler des recommandations sur les façons d'améliorer le système de santé. Notre analyse d'entrevues menées auprès de membres et de responsables d'organismes consultatifs (p. ex., représentants, employés et consultants du ministère de la Santé) vise à savoir pourquoi les personnes interviewées estiment que leurs conseils et recommandations ne sont généralement pas mis en œuvre et pourquoi des groupes de stratégie informels sont employés pour faciliter la mise en œuvre. Nous recommandons que les éventuels organismes consultatifs du système de santé se concentrent sur la formation de coalitions lors de l'élaboration des politiques, intègrent les plans de mise en œuvre dans les recommandations d'ordre politique et en évaluent l'impact.
About the Author(s)
Amity E. Quinn, Phd, Assistant Professor, Department of Obstetrics & Gynecology and Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB
Rachelle Drummond, MPP, MSC, Research Associate, O'Brien Institute for Public Health, University of Calgary, Calgary, AB
Tom Noseworthy, MD, MPH, Professor Emeritus, Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB
Fiona Clement, Phd, Professor and Head, Department of Community Health Science, Cumming School of Medicine University of Calgary, Calgary, AB
Stephana Moss, Phd, Assistant Professor, Department of Pediatrics Dalhousie University, Halifax, NS
Emily Fitzgerald, MA, Phd Student Harvard T.H. Chan School of Public Health Boston, MA, US
Melanie Columbus, Phd, Managing Director, Centre for Health Policy O'Brien Institute for Public Health University of Calgary, Calgary, AB
Brenlea Farkas, MSC, Senior Research Associate, Centre for Health Policy O'Brien Institute for Public Health, University of Calgary, Calgary, AB
Henry T. Stelfox, MD, Phd, Deputy Dean, Faculty of Medicine & Dentistry University of Alberta Edmonton, AB, Adjunct Professor, Department of Critical Care Medicine, Cumming School of Medicine University of Calgary Calgary, AB
References
Advisory Council on the Implementation of National Pharmacare. 2019, June. A Prescription for Canada: Achieving Pharmacare for All: Final Report of the Advisory Council on the Implementation of National Pharmacare. Government of Canada. Retrieved March 11, 2025. <https://www.canada.ca/content/dam/hc-sc/images/corporate/about-health-canada/public-engagement/external-advisory-bodies/implementation-national-pharmacare/final-report/final-report.pdf>.
Advisory Panel on Healthcare Innovation. 2015, July. Unleashing Innovation: Excellent Healthcare for Canada: Report of the Advisory Panel on Healthcare Innovation. Health Canada Ottawa. Retrieved March 11, 2025. <https://healthycanadians.gc.ca/publications/health-system-systeme-sante/report-healthcare-innovation-rapport-soins/alt/report-healthcare-innovation-rapport-soins-eng.pdf>.
Braun, V. and V. Clarke. 2006. Using Thematic Analysis in Psychology. Qualitative Research in Psychology 3(2): 77–101. doi:10.1191/1478088706qp063oa.
Braun, V. and V. Clarke. 2019. Reflecting on Reflexive Thematic Analysis. Qualitative Research in Sport, Exercise and Health 11(4): 589–97. doi:10.1080/2159676X.2019.1628806.
Bullock, H.L., J.N. Lavis, M.G. Wilson, G. Mulvale and A. Miatello. 2021. Understanding the Implementation of Evidence-Informed Policies and Practices From a Policy Perspective: A Critical Interpretive Synthesis. Implementation Science 16(1): 18. doi:10.1186/s13012-021-01082-7.
Butterfoss, F.D., R.M. Goodman and A. Wandersman. 1996. Community Coalitions for Prevention and Health Promotion: Factors Predicting Satisfaction, Participation, and Planning. Health Education Quarterly 23(1): 65–79. doi:10.1177/109019819602300105.
Byrne, D. 2022. A Worked Example of Braun and Clarke's Approach to Reflexive Thematic Analysis. Quality and Quantity 56(3): 1391–412. doi:10.1007/s11135-021-01182-y.
Canada Health Act (R.S.C. 1985, c. C-6). Government of Canada. Retrieved March 11, 2025. <https://laws-lois.justice.gc.ca/eng/acts/c-6/>.
Commission on the Future of Health Care in Canada. 2002, November. Building on Values: The Future of Health Care in Canada: Final Report. Retrieved March 11, 2025. <https://publications.gc.ca/collections/Collection/CP32-85-2002E.pdf>.
Constitution Act, 1867 (UK), 30 & 31 Vict, c 3, reprinted in RSC 1985, App II, No 5. Government of Canada. Retrieved March 11, 2025. <https://canlii.ca/t/56g8v>.
Halffman, W. and R. Hoppe. 2005. Science/Policy Boundaries: A Changing Division of Labour in Dutch Expert Policy Advice. In S. Maasen and P. Weingart, eds., Democratization of Expertise? (pp. 135–51). Springer.
Health Ministers of Canada. 2004. A 10-year Plan to Strengthen Health Care. Government of Canada. Retrieved March 11, 2025. <https://www.canada.ca/en/health-canada/services/health-care-system/health-care-system-delivery/federal-provincial-territorial-collaboration/first-ministers-meeting-year-plan-2004/10-year-plan-strengthen-health-care.html>.
Lennox, L., C. Doyle, J.E. Reed and D. Bell. 2017. What Makes a Sustainability Tool Valuable, Practical and Useful in Real-World Healthcare Practice? A Mixed-Methods Study on the Development of the Long Term Success Tool in Northwest London. BMJ Open 7(9): e014417. doi:10.1136/bmjopen-2016-014417.
Lindquist, E.A. 1993. Think Tanks or Clubs? Assessing the Influence and Roles of Canadian Policy Institutes. Canadian Public Administration 36(4): 547–79. doi:10.1111/j.1754-7121.1993.tb00833.x.
Lumivero. 2017. NVivo (Version 12). <https://www.lumivero.com>.
Matland, R.E. 1995. Synthesizing the Implementation Literature: The Ambiguity-Conflict Model of Policy Implementation. Journal of Public Administration Research and Theory 5(2): 145–74. doi:10.1093/oxfordjournals.jpart.a037242.
McIntosh, T. and P.G. Forest. 2010. Talking To and With Canadians: Citizen Engagement and the Politics of the Romanow Commission. Southern Journal of Canadian Studies 3(1): 28–50. doi:10.22215/sjcs.v3i1.275.
Medical Care Act (R.S.C. 1966, c. M-6). Government of Canada. Retrieved March 11, 2025. <https://publications.gc.ca/collections/collection_2024/edsc-esdc/R44-159-1967-eng.pdf>.
Milat, A., K. Lee, K. Conte, A. Grunseit, L. Wolfenden, F. van Nassau et al. 2020. Intervention Scalability Assessment Tool: A Decision Support Tool for Health Policy Makers and Implementers. Health Research Policy and Systems 18: 1. doi:10.1186/s12961-019-0494-2.
Mintrom, M., D. O'Neill and R. O'Connor. 2021. Royal Commissions and Policy Influence. Australian Journal of Public Administration 80(1): 80–96. doi:10.1111/1467-8500.12441.
National Forum on Health. 1997. Canada Health Action: Building on the Legacy – Volume I – The Final Report. Government of Canada. Retrieved March 11, 2025. <https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-renewal/canada-health-action-building-legacy-volume1.html>.
Standing Senate Committee on Social Affairs. 2002. The Health of Canadians, the Federal Role. Volume Six: Recommendations for Reform/The Honourable Michael J.L. Kirby, Chair; the Honourable Marjory LeBreton, Deputy Chair. Government of Canada. Retrieved March 11, 2025. <https://publications.gc.ca/site/eng/398166/publication.html>.
Task Force on Cannabis Legalization and Regulation. 2016, November 30. A Framework for the Legalization and Regulation of Cannabis in Canada: The Final Report of the Task Force on Cannabis Legalization and Regulation. Government of Canada. Retrieved March 11, 2025. <https://www.canada.ca/content/dam/hc-sc/healthy-canadians/migration/task-force-marijuana-groupe-etude/framework-cadre/alt/framework-cadre-eng.pdf>.
Zegart, A.B. 2004. Blue Ribbons, Black Boxes: Toward a Better Understanding of Presidential Commissions. Presidential Studies Quarterly 34(2): 366–93. doi:10.1111/j.1741-5705.2004.00049.x.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed