
Healthcare Policy
Abstract
People experiencing infertility often face challenges accessing treatment, such as in vitro fertilization (IVF), especially in contexts where treatments are not funded by government or public health insurance plans. Using an original survey, this paper examines barriers to accessing IVF in British Columbia (BC), a province that recently announced that it would start funding IVF, beginning in fiscal year 2025/26. The survey findings highlight the financial, geographic and personal barriers that limit access to treatment. BC's new publicly funded IVF program should address patient challenges related to upfront costs, regional variation in the unaffordability of treatment and existing research related to embryo transfer limits in other provinces.
Introduction
Canada is experiencing a decrease in its average fertility rate while also seeing increasingly older first-time parents and growing rates of age-related infertility. Alongside these changes, advances in medical technology since the 1980s have made access to fertility treatments a possible solution for those living with infertility. For those living with infertility, in vitro fertilization (IVF) is one such medical intervention that can help make parenthood a reality. This development in reproductive technologies and changing fertility patterns has spurred an increased demand for fertility interventions and services, where IVF pregnancies and births have increased by 20% since 2013 (CARTR-Plus and BORN Ontario 2024). However, the costs of IVF (ranging from $10,000–$20,000 per cycle) can be prohibitive, and as a matter of healthcare, the decision whether to cover the costs of the service falls to individual provinces.
While the federal government provides funding through the Canada Health Transfer (Tiedemann 2019) and requires provinces and territories to uphold the principles of universality, as outlined in the Canada Health Act (1984), provinces and territories are empowered to choose what is covered in their health insurance programs and whether they fund health services through other means, as Ontario does with its IVF program that operates outside of the Ontario Health Insurance Plan (Cantor et al. 2023). This results in variation not only in what patients have access to but also in how provinces and territories determine what health policy agendas to adopt and how best to implement them. This process, namely, policy divergence and incoherence in the context of federalism, is well documented in the literature (Béland et al. 2024; Marchildon and Bossert 2018; Palley and Forest 2004). However, there is little research that seeks to understand the actual impacts of policy variation from the perspectives and lived experiences of the users impacted by these differing policy approaches, especially as they relate to healthcare decisions in provinces without funding or policy intervention.
While several provinces offer some form of funding for IVF, ranging from funded cycles to tax credits, others provide no public coverage for the treatment (Austin and Apold 2023; Snow 2018). As a result, accessing treatment in provinces without funding coverage can be difficult (Mounce et al. 2022). Barriers to accessing IVF may vary, and understanding what affects the accessibility of IVF can offer insight to provincial policy makers as they continue to develop IVF and other related fertility treatment policies. To this end, this study asks what barriers prevent people in British Columbia (BC) from accessing IVF services and what challenges they face when they do access treatment. The objective of this paper is to highlight the challenges faced by those experiencing infertility in BC at a time when the province was not yet funding IVF or other fertility treatments. BC has recently announced that it would begin funding “one cycle of IVF for eligible B.C. residents” in the 2025–26 fiscal year. As the policy is still being developed, understanding the barriers that have limited access to those experiencing infertility can support improved policy design while encouraging policy makers to account for variable barriers across different regions in the province.
Methods
Study design
To study the barriers that affect people in BC trying to access IVF services, this study includes an anonymous, online survey of more than 200 self-identified women engaged with either fertility clinics or online support groups for those experiencing infertility. The themes and design of the survey are informed by a preliminary literature review where both academic literature and clinical reports inform survey questions and capture considerations for policy design, such as access, barriers, outcomes and demographics with the goal of better understanding the lived experience of those seeking IVF. The survey is designed to identify demographic trends, variable barriers to access, average costs to patients, presence of insurance coverage, regional gaps in access, etc. Furthermore, the survey includes questions related to patterns in embryo transfers and multiple births to provide policy makers with the experience of those who have been able to access IVF in BC ahead of the funding rollout in 2025. Participants were asked a total of 28 questions (Appendix A, available online here) with the option to provide open-ended text responses to allow respondents to identify barriers or policy considerations not otherwise raised throughout the survey. In order to ascertain specific answers from those participants who have not undergone IVF, compared with those who have undergone the process or who may have been undergoing IVF while participating, a skip logic function is used, meaning that depending on a respondent's answer, they were redirected to specific questions.
Recruitment
Survey participants include self-identified women in BC experiencing infertility who are pursuing IVF and those who are not able to pursue it due to barriers. To ensure regional representation, the survey was distributed in partnership with three fertility clinics across the province, including in areas without IVF clinics, such as Northern BC. The clinics displayed the recruitment poster (Appendix B, available online here), which featured a QR code, in their offices and waiting rooms, allowing clients/patients to complete the survey while accessing these services. Recruitment was also done in partnership with two BC-specific fertility support groups on Facebook with permission from the groups' moderators. One of the groups had upwards of 900 members while the other had just under 300 members. Lastly, several fertility coaches posted the recruitment poster to their web pages and social media platforms, including Facebook and Instagram.
Data collection and analysis
The data were captured via SurveyMonkey, an online survey platform, in the winter of 2020. The survey was open for approximately two months. Data were analyzed using descriptive analysis in Excel to capture trends and create data visualizations. In addition to the multiple-choice survey questions, qualitative responses were captured via a single open-ended question: “Should you wish to expand on any responses or general themes as they relate to this survey, please do so in the text box below”. These responses, of which there are more than 100 across subgroups, were coded manually via the constant comparison method (Strauss and Corbin 1990) for thematic analysis to capture similar responses and better understand access barriers and perceived policy preferences among survey participants.
Results
Sample description
While 253 respondents accessed and consented to the survey, only 203 completed it in its entirety, including all demographical questions. Given the importance of understanding demographical trends and how access to IVF varies by socio-economic status, region, marital status, etc., only complete surveys are included in the analysis, resulting in a sample of 203. Table 1 highlights respondents' socio-demographic characteristics and their general experience with IVF and infertility.
| TABLE 1. Characteristics of survey participants | ||||||
| Sample description | All respondents (n = 203) | |||||
| IVF access |
|
|||||
| Infertility |
|
|||||
| Age groups of participants |
|
|||||
| Combined household income |
|
|||||
| Education |
|
|||||
| Employment |
|
|||||
| Partnership status |
|
|||||
| Community type |
|
|||||
| Regional representation |
|
|||||
Respondents who have not undergone IVF
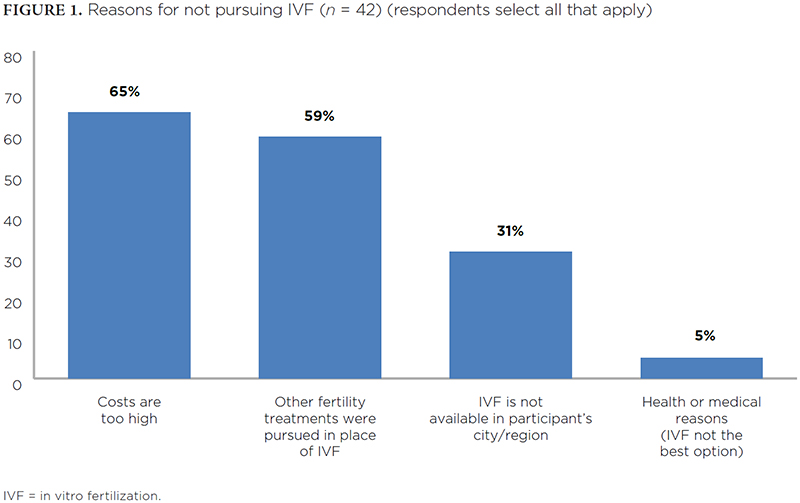
Examining the 42 respondents who have not yet undergone IVF reveals key access barriers for policy makers to consider. First, regional variation exacerbates the inaccessibility of IVF; of all respondents from the Thompson-Okanagan region, 37% indicated having not undergone IVF, with all of these respondents indicating that it was due to cost and geographical constraints. Similarly, 32% of Northern BC respondents indicated not having undergone IVF. These figures for these two regions exceed both the sample average of 21% and the Lower Mainland respondents' figure of only 14%.
Beyond geographical barriers, the reasons for respondents not pursuing IVF point to important policy considerations around patient costs and what the impact of alternative funding options may hold. For instance, of all respondents unable to pursue IVF, 79% indicated that if the service were publicly funded, they would have undergone the procedure. When asked to indicate all reasons for not undergoing IVF, meaning participants could select more than one answer, 64% of respondents indicated that the costs were too high, while 31% indicated that IVF is not offered in their city or region (Figure 1).1
{kind=link}

Participants who indicated having not undergone IVF are also provided with the opportunity to expand on what factors limit access and how policy might address these gaps. The qualitative results also demonstrate that, beyond costs being a determining factor in not pursuing treatment, they also impact a respondent's decision to pursue other medical interventions. As demonstrated by the respondent quotes below, the financial aspects of IVF can push patients to alternative treatments, such as intrauterine insemination (IUI), with the view being that it is less effective. This has important implications not only for patient autonomy but also because the pursuit of less effective treatment may result in even older patients requiring assisted reproductive technology, having not had a pregnancy through initial, less expensive interventions.
We are pursuing IUI before IVF because it [IVF] is too expensive even though it's more successful.
I have stage two endometriosis and my partner has Male Factor Infertility. We have been recommended to pursue IVF + ICSI but the base cost is $8,500 plus medications, and we don't have that amount saved up … We have been devastated by our diagnoses and the lack of funding for medical treatment.
Respondents Pursuing IVF or Who Previously Underwent IVF
The 161 respondents who either previously underwent IVF or who are pursuing IVF were asked about access and, similar to the challenges that restrict access for those who have not pursued IVF, 81% of respondents indicated experiencing financial barriers. This is also reflected in participants' reported total costs of IVF, with nearly 40% of respondents having spent upward of $28,000, some of whom indicated spending up to $150,000–$200,000. It may be the case that for these extremely high-cost figures, some patients may be including associated expenses such as egg freezing, egg or sperm donations, surrogacy, etc. Furthermore, 63% of these respondents indicated that they would have undergone additional cycles if IVF was publicly funded. A summary of findings for this group of respondents can be found in Table 2.
| TABLE 2. Findings for those who have undergone or who are pursuing IVF | ||||||
| Sample description | Respondents pursuing or who have undergone IVF (n = 161) | |||||
| Reported costs for IVF | 11% (18 respondents) have spent between $7,000 and $13,999 30% (48 respondents) have spent between $14,000 and $20,999 20% (32 respondents) have spent between $21,000 and $27,999 22% (35 respondents) have spent between $28,000 and $49,999 17% (27 respondents) have spent more than $50,000, with some respondents indicating total costs of up to $150,000 and $200,000 |
|||||
| Reported insurance coverage for IVF medications | 34% (55 respondents) have no insurance coverage for IVF medications 58% (93 respondents) have partial coverage for IVF medications 8% (13 respondents) have full coverage for IVF medications |
|||||
| Reported insurance coverage for IVF | 96% (155 respondents) have no insurance coverage for IVF 4% (6 respondents) have partial coverage for IVF |
|||||
| Barriers (respondents select all that apply) | 81% (130 respondents) indicated experiencing financial barriers 55% (89 respondents) indicated experiencing emotional barriers 35% (56 respondents) indicated experiencing workplace challenges 25% (40 respondents) indicated experiencing geographical barriers 16% (26 respondents) indicated experiencing health and physical barriers 9% (14 respondents) indicated experiencing no barriers to accessing IVF |
|||||
| IVF = in vitro fertilization. | ||||||
With minimal insurance coverage available for treatment, as noted in the survey responses, these costs have important implications not only for those who cannot afford IVF but also for how those who can afford it choose to pay for it. Beyond the sheer cost of treatment, respondents also indicated that the associated financial barriers often required them to delay treatment to save, or that they look to other options such as support from parents, remortgaging their homes, lines of credit or online fundraisers such as “GoFundMe” to cover the costs, as evidenced by the qualitative responses below. This raises important questions regarding not only income equity but also what other decisions may be impacted by the high upfront costs of IVF, including whether to pursue other forms of treatment, impacts on other health concerns or whether a patient may have to stop treatment altogether due to costs.
Due to financial restrictions, we had to wait six years to be able to afford to do the second transfer of our final frozen embryo.
Because of the financial barriers, we tried multiple rounds of IUI before moving to IVF.
While only 25% of respondents in this subgroup indicated geographical barriers, it is noteworthy, though unsurprising, that when isolating for regions, geographical barriers are selected by 96% of Northern BC respondents and 48% of Thompson-Okanagan respondents compared with only 9% of Lower Mainland respondents. As evidenced by the following quotes, the travel time and costs can be burdensome, adding additional barriers to those living in regions without full-service IVF clinics. It is also important to consider the fact that as IVF is not a one-time “procedure,” but instead a series of consultations, monitoring appointments, transfers and check-ups, the scheduling challenges can exacerbate geographic barriers.
No clinics are located in Northern BC, so we had to relocate to Vancouver for two weeks while undergoing stims/retrieval/transfer.
My husband and I can't afford to both travel for the procedure, so I will be going alone.
Looking at outcomes for those respondents who are either pursuing or who have previously pursued IVF, 34% indicated having completed more than two cycles, which includes all retrievals and transfers. When looking more specifically at embryo transfers, we see that experiences vary for those respondents who have undergone different numbers of transfers. For this aspect of the survey, respondents were first asked how many transfers they had undergone, then asked the maximum number of embryos transferred. Of those participants who have only undergone one transfer, 37% indicated having had a multiple embryo transfer during that initial cycle compared with 47% for those who have undergone two transfers (Table 3). Of all 141 respondents who have undergone IVF, only 14% (20 respondents) indicated having given birth to multiples. When looking at these births of multiples among only those 75 respondents who have experienced the birth of one or more babies as a result of IVF, this figure climbs to 28% (Table 3).
| TABLE 3. Summary of embryo transfers and birth outcomes for respondents who have undergone at least one IVF cycle | ||||||
| Sample description | Respondents who have undergone IVF (n = variable depending on the number of transfers) |
|||||
| IVF outcomes | Of the 141 respondents who have undergone at least one IVF cycle:
|
|||||
| Birth outcomes | Of the 75 respondents who have experienced the birth of one or more babies as a result of IVF:
|
|||||
| Embryo transfers | Of the 51 respondents who have completed only one embryo transfer:
Of the 30 respondents who have undergone two embryo transfers:
Of the 69 respondents who have undergone more than two embryo transfers:
|
|||||
Discussion
As shown in the survey data, there are significant and inequitable barriers limiting access to IVF in BC. While BC has announced that it intends to launch its program, which will provide funding for one cycle of IVF for eligible BC residents, beginning in the 2025–26 fiscal year, there are ongoing considerations that policy makers should review. In particular, three considerations evidenced in the survey data should be examined in program design: perceptions around infertility as a medical concern and patient perspectives on funding; demographic and equity considerations for accessing IVF; and regulatory considerations as they relate to embryo transfer policies.
Looking first at infertility as a healthcare issue and the associated demand for eligibility, policy makers might consider the medicalization of infertility and the perception of those undergoing IVF. In particular, the thematic analysis reveals a consistent view of infertility being a medical condition with available treatment options. As is, private funding models contribute to the continued financialization of reproductive care and limit access by social status, income, and region and, as some have argued, delegitimize infertility as a medical issue worthy of funding (Bell 2016; Jain 2006; Shanley and Asch 2009). While some respondents have the option of pursuing alternative interventions such as IUI, which can be effective for male factor infertility, those experiencing more complex forms of infertility are faced with fewer choices. As such, the cost of IVF can act as a prohibitive barrier for those requiring more specialized treatment, such as intracytoplasmic sperm injection (ICSI), a treatment typically used in association with severe male factor infertility (Khatun et al. 2018).
These financial barriers faced by respondents also differ by region, with housing prices and workplace opportunities effectively preventing those with some types of medical infertility from accessing the necessary treatment or from putting money toward savings or other areas. As such, policy makers might consider funding options that ensure demographical equity. As the purpose of this paper was to identify barriers to accessing IVF, it follows that there are unique barriers to account for within BC. In particular, regional barriers and the challenges of upfront costs are likely to continue barring patients outside of the lower mainland from access. Given the laboratory infrastructure and massive investments required, developing complete IVF services in Northern BC, the Okanagan and the Kootenays remains unlikely and perhaps, unnecessary. Instead, policy makers might consider funding options that facilitate travel to those areas offering IVF. Though BC has recently confirmed that its program will provide funding for one cycle of IVF for eligible residents, policy makers should consider additional funding coverage for those outside of the lower mainland or those in areas without IVF clinics. Otherwise, the program risks continued exclusion based on region and costs associated with travel. Options such as a fertility grant or special assistance fund could alleviate some of the regional barriers while enabling pre-treatment allowances, thereby reducing some of the obstacles associated with the upfront expenses. The strength of this funding model lies in the certainty of costs for the government compared with a rolling fertility program, similar to that seen earlier in Quebec before the province replaced funded cycles with a refundable tax-credit model (Shaulov et al. 2015). Furthermore, the income and regional equity delivered via ex-ante funding coverage coupled with the ease of implementation, as demonstrated by New Brunswick's success with its earlier special assistance fund, is another highlight of this type of funding model.
Finally, beyond considering barriers to accessing IVF and which funding model might best meet budgetary needs, policy makers might consider regulatory reform once IVF is funded by the government. As noted throughout the literature, there are health risks to both pregnancies and births associated with multiples, including premature delivery, jaundice, low birth weight, preeclampsia, gestational diabetes and peripartum hemorrhage, among others (Attawet et al. 2022; Bergh et al. 2020; El-Toukhy et al. 2018; Sazonova et al. 2013). This highlights a critical aspect of policy consideration, where at a national level, there are calls for reducing multiple births associated with IVF (CARTR-Plus and BORN Ontario 2024), yet provinces without such regulations, chiefly those without publicly funded IVF, may continue to face challenges associated with multiple births (El-Toukhy et al. 2018; Lanes et al. 2020; Van Voorhis and Ryan 2010). While the scope of this study is relatively narrow, and the results related to multiple births should not be overstated, the survey findings suggest that this aspect of IVF policy development is an area for further research and monitoring as BC develops its funding model. BC could consider reviewing existing provincial policies across Canada to examine the impacts of attaching a single embryo transfer guideline to its program, as is the case in other provinces.
Conclusion
By bringing together patients undergoing IVF and those hoping but unable to access treatment, this study has sought to identify barriers that affect British Columbians looking for IVF. These results are particularly timely as they highlight critical considerations for BC's recently announced fertility program. In particular, the lived experience of those dealing with infertility reaffirms the need for such a program while highlighting critical policy considerations such as ex-ante financial barriers, regional inequities and pregnancy and birth outcomes that merit further research. Though BC has until recently been an outlier among its peer provinces for its lack of funding for IVF, the province now has the opportunity to learn from jurisdictions with both successful programs and those that struggled with earlier rollouts. In developing this new program, policy makers should be cognizant of the critical access barriers that go beyond costs and ensure that the funding instrument alleviates barriers related to BC's geography, the upfront costs and treatment, the challenges of lottery or waitlist systems managed by private clinics and the previously identified risks associated with an elevated multiple births rate.
Correspondence may be directed to Jenna Quelch by e-mail at jenna.quelch@mail.utoronto.ca.
Ethics Approval and Consent to Participate
The study was approved by the Simon Fraser University Office of Research Ethics. Informed consent was obtained from all individual study participants.
Conception de politiques : point de vue des femmes qui ont recours à la FIV en Colombie-Britannique
Résumé
Les personnes souffrant d'infertilité ont souvent du mal à accéder aux traitements comme la fécondation in vitro (FIV), en particulier là où les traitements ne sont pas financés par le gouvernement ou par les régimes publics d'assurance maladie. À l'aide d'un sondage original, ce document examine les obstacles à l'accès à la FIV en Colombie-Britannique (C.-B.), une province qui a récemment annoncé qu'elle commencerait à financer la FIV à partir d'avril 2025. Les résultats de l'enquête mettent en évidence les obstacles financiers, géographiques et personnels qui limitent l'accès au traitement. Le nouveau programme de FIV financé par les deniers publics de la C.-B. devrait répondre aux défis que rencontrent les patients en matière de coûts initiaux, de variation régionale du caractère inabordable du traitement et de recherches existantes liées aux limites de transfert d'embryons dans d'autres provinces.
About the Author(s)
Jenna Quelch, MPP, Phd Candidate, Department of Political Science, Dalla Lana School of Public Health, University of Toronto, Toronto, ON
References
Attawet, J., A.Y. Wang, C.M. Farquhar, V. Jordan, Z. Li and E.A. Sullivan. 2022. Pregnancy and Birth Outcomes of Single Versus Multiple Embryo Transfer in Gestational Surrogacy Arrangements: A Systematic Review and Meta-Analysis. Human Fertility 25(2): 217–27. doi:10.1080/14647273.2020.1785643.
Austin, N. and V. Apold. 2023. Canadian Access to Assisted Reproduction: Mapping Changes Over Time. Journal of Obstetrics and Gynaecology Canada 45(9): 644–45. doi:10.1016/j.jogc.2023.04.024.
Béland, D., G.P. Marchildon, A. Medrano and P. Rocco. 2024. Policy Feedback, Varieties of Federalism, and the Politics of Health-Care Funding in the United States, Mexico, and Canada. Politics and Policy 52(1): 51–69. doi:10.1111/polp.12575.
Bell, A.V. 2016. The Margins of Medicalization: Diversity and Context Through the Case of Infertility. Social Science and Medicine 156: 39–46. doi:10.1016/j.socscimed.2016.03.005.
Bergh, C., M.S. Kamath, R. Wang and S. Lensen. 2020. Strategies to Reduce Multiple Pregnancies During Medically Assisted Reproduction. Fertility and Sterility 114(4): 673–79. doi:10.1016/j.fertnstert.2020.07.022.
Canada Health Act (R.S.C., 1985, c. C-6). Government of Canada. Retrieved April 25, 2025. <https://laws-lois.justice.gc.ca/eng/acts/c-6/>.
CARTR-Plus and BORN Ontario. 2024. Canadian Assisted Reproductive Technologies Register (CARTR) Plus Annual Report. Canadian Fertility and Andrology Society. Retrieved April 25, 2025. <https://cfas.ca/_Library/CARTR/2024_CARTR_annual_report_CFAS.pdf>.
Cantor, A., L. Meng, A. Lanes and E.M. Greenblatt. 2023. The Effect of the Ontario Fertility Program on IVF Utilization and Outcomes in Women of Advanced Reproductive Age. Reproductive Biomedicine Online 46(2): 410–16. doi:10.1016/j.rbmo.2022.05.014.
Collins, J.A. 2002. An International Survey of the Health Economics of IVF and ICSI. Human Reproduction Update 8(3): 265–77. doi:10.1093/humupd/8.3.265.
El-Toukhy, T., S. Bhattacharya and V. Akande. 2018. Multiple Pregnancies Following Assisted Conception: Scientific Impact Paper No. 22. International Journal of Obstetrics and Gynaecology 125(5): e12–18. doi:10.1111/1471-0528.14974.
HealthLinkBC. 2021. Infertility: Setting Limits on Treatment. Retrieved April 25, 2025. <https://www.healthlinkbc.ca/healthwise/infertility-setting-limits-treatment>.
Jain, T. 2006. Socioeconomic and Racial Disparities Among Infertility Patients Seeking Care. Fertility and Sterility 85(4): 876–81. doi:10.1016/j.fertnstert.2005.07.1338.
Khatun, A., M.S. Rahman and M.-G. Pang. 2018. Clinical Assessment of the Male Fertility. Obstetrics and Gynecology Science 61(2): 179–91. doi:10.5468/ogs.2018.61.2.179.
Lanes, A., D.B. Fell, M. Teitelbaum, A.E. Sprague, M. Johnson, H. Wang et al. 2020. CARTR Plus: The Creation of an ART Registry in Canada. Human Reproduction Open 2020(3): hoaa022. doi:10.1093/hropen/hoaa022.
Marchildon, G.P. and T.J. Bossert. 2018. Federalism and Decentralisation in Health Care: A Decision Space Approach. University of Toronto Press.
Mounce, G., H.T. Allan and N. Carey. 2022. “Just Have Some IVF!”: A Longitudinal Ethnographic Study of Couples' Experiences of Seeking Fertility Treatment. Sociology of Health and Illness 44(2): 308–27. doi:10.1111/1467-9566.13429.
Palley, H.A. and P.-G. Forest. 2004. Canadian Fiscal Federalism, Regionalization, and the Development of Quebec's Health Care Delivery System. New Global Development 20(2): 87–96. doi:10.1080/17486830408417014.
Sazonova, A., K. Källen, A. Thurin-Kjellberg, U.-B. Wennerholm and C. Bergh. 2013. Neonatal and Maternal Outcomes Comparing Women Undergoing Two In Vitro Fertilization (IVF) Singleton Pregnancies and Women Undergoing One IVF Twin Pregnancy. Fertility and Sterility 99(3): 731–37. doi:10.1016/j.fertnstert.2012.11.023.
Shanley, M.L. and A. Asch. 2009. Involuntary Childlessness, Reproductive Technology, and Social Justice: The Medical Mask on Social Illness. Signs: Journal of Women in Culture and Society 34(4): 851–74. doi:10.1086/597141.
Shaulov, T., S. Belisle and M.H. Dahan. 2015. Public Health Implications of a North American Publicly Funded In Vitro Fertilization Program; Lessons to Learn. Journal of Assisted Reproduction and Genetics 32(9): 1385–93. doi:10.1007/s10815-015-0530-2.
Snow, D. 2018. Assisted Reproduction Policy in Canada: Framing, Federalism, and Failure. University of Toronto Press.
Strauss, A. and J. Corbin. 1990. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Sage.
Tiedemann, M. 2019. The Canada Health Act : An Overview / Marlisa Tiedemann.: YM32-2/2019-54E-PDF - Government of Canada Publications - Canada.ca. Retrieved November 20, 2023. <https://publications.gc.ca/site/eng/9.892172/publication.html>.
Van Voorhis, B.J. and G.L. Ryan. 2010. Ethical Obligation for Restricting the Number of Embryos Transferred to Women: Combating the Multiple-Birth Epidemic From In Vitro Fertilization.
Footnotes
1. It should be noted that for the 5% (2 respondents among 42) who indicated not pursuing IVF due to health or medical reasons where IVF is not the best option, it may be the case that they are pursuing IUI with the view they may pursue IVF later, or perhaps they had previously undergone IVF and have discontinued. In both cases, this subset of respondents presents a limitation to the paper as further probing is not feasible. It may be the case that they participated in the survey given other conditions related to infertility and reproductive healthcare (e.g., while visiting a clinic for other services).
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed