
Healthcare Policy
Health Worker Protests in Canada: A Descriptive Analysis of Protest Events from 2021-2022
Veena Sriram, Meena Rakasi, Kartik Sharma, Michael R. Law and Sorcha A. Brophy
Abstract
Objectives: We analyzed protest events undertaken by health workers in Canada in 2021 and 2022. Our analysis focused on the quantity and distribution of protests within Canada, policy demands expressed by organizers and the temporal sequence of protest events.
Methods: Our data came from the Armed Conflict Location and Event Data (ACLED) project, which includes a dataset with all health worker-involved protest events in specific jurisdictions, including Canada. Using an existing taxonomy of policy demands for protest events, we analyzed specific types of protests, protest demands and temporal trends.
Results: Over our study period, ACLED identified 157 health worker protests. Events took place in all provinces, with Ontario recording the highest proportion (~40%). The majority of protests focused on working conditions and remuneration (57%), followed by public policy (26%) and health services delivery (21%). The most frequent subcategories were compensation (n = 48), anti-vaccination mandates (n = 38) and understaffing/patient overload (n = 19).
Conclusion: Canadian health workers expressed concerns on policy issues ranging from opposition to COVID-19 mitigation to underinvestment in health systems. Identifying and recognizing these drivers and developing targeted policy to address them through inclusive and sustained engagement with health workers will contribute to long-term solutions.
Introduction
The roles and influence of health workers in health policy processes – and public policy more broadly – are gaining increasing attention in health scholarship (Ahmed et al. 2022). Representative health worker organizations, such as unions and professional associations, play a key role in health policy processes, facilitating dialogue between government, employers and health workers (Sriram et al. 2023). Furthermore, health worker engagement with policy processes through activities such as voting, organized lobbying, collective bargaining and protest activity plays an important role in shaping public policy (Sriram et al. 2023). These activities have implications beyond labour concerns, including patient well-being, healthcare financing, resource allocation and other public health, healthcare and public policy domains (Brophy and Sriram 2021; Lasco et al. 2022; Laugesen 2019). A current strand of research has sought to understand the political preferences of health workers – especially physicians (Ahmed et al. 2022; Bonica et al. 2014; Jena et al. 2018). Simultaneously, recent research on the politics of representative health worker organizations in more diverse contexts than previously studied has begun to theorize about the strategies used by these organizations to advance their policy agendas (Brophy and Sriram 2021; Sriram et al. 2023). Still, many questions remain regarding policy preferences within and across the health workforce and the modes by which health workers make those preferences known (Hagedorn et al. 2016).
Health workers belong to a heterogeneous group of occupations (including those delivering clinical care such as doctors and nurses as well as those delivering non-clinical services such as long-term care workers and custodial staff) with diverse concerns and demands regarding both the conditions of their occupations and larger healthcare systems (WHO 2019). Protests and strike action are an important window into understanding the policy preferences of various constituencies of health workers. The use of protest and strike action by health workers in particular has received greater public attention due to the COVID-19 pandemic. Since the earliest stages of the pandemic, numerous countries experienced protests and strikes led by health workers calling for improved compensation and benefits, better working environments and resources needed to perform their roles (Brophy et al. 2022; Mavis Mulaudzi et al. 2021; Trappman et al. 2022). Beyond the specific challenges imposed by COVID-19, protests and strikes signalled that health workers have wide-ranging grievances and concerns about issues including (but not limited to) healthcare systems, public health and public policy (Jane et al. 2022).
Canada – similar to countries around the world – is experiencing a health workforce crisis. Employment vacancies in the healthcare sector have been high, particularly in nursing and residential care facilities (Drummond et al. 2022). The impacts of COVID-19 on health workers in Canada include immediate concerns related to pandemic response (i.e., resource constraints and safety concerns) as well as longer-term challenges (i.e., declining trust in healthcare and scientific expertise). The pandemic also exacerbated workforce and system delivery challenges in health sectors across Canada. For example, in April 2020, the Canadian Armed Forces were deployed to senior care facilities in Ontario and Quebec to assist medical care and support staff who were overwhelmed by the onset of the pandemic in the midst of a workforce crisis and reported dire conditions in the facilities (Brewster and Kapelos 2020). Attrition within the workforce is increasing, as practitioners exit the workforce in part due to burnout (Drummond et al. 2022; Duong and Vogel 2023; Gajjar et al. 2022; Leo et al. 2021), compensation, understaffing and challenging working conditions (Drummond et al. 2022; Stewart 2022), which were concerns driven by or made worse due to the pandemic. Some health workers are exiting the public sector to pursue employment in private agency staffing models (Grant 2023), contributing to ongoing constraints and challenges with health worker supply (Drummond et al. 2022). These trends have been fuelled by public policy decisions – several of which predate the pandemic – that have negatively impacted health workers' remuneration, benefits and job security. For example, the Ontario government passed Bill 124 in 2019, which limited public sector wage increases to 1% per year for three years (Jones 2019), prompting legal action and protests by public sector employees, including health workers (Wilson 2022).
It has become increasingly apparent that more research is needed to understand the policy demands of health workers in Canada within a global context. The health workforce crisis in Canada has ripple effects on other countries; migration of internationally trained health workers, largely from the Global South, to Canada has been actively promoted as a policy solution to addressing the national shortage (Government of Canada 2023; Tasker 2023), creating challenges for resource-constrained countries experiencing their own workforce shortages (WHO 2023). The World Health Organization has estimated that there will be a global shortage of 10 million health workers by 2030, primarily in low- and middle-income countries (WHO n.d.). Policy issues that demand collective action and global solidarity, such as the climate crisis and racial injustice, have also recently become more prominent in the advocacy of Canadian health workers (Jane et al. 2022; Kalifa et al. 2022).
Approximately 54% of Canadian health workers are unionized (Statistics Canada 2024), with heterogeneity across occupational groups. Canadian health workers have a long history of engaging in resistance, including protests and strikes (both legally sanctioned and non-sanctioned) (Heron and Smith 2020). For example, doctors in Saskatchewan organized a 23-day strike in 1962 in opposition to single-payer health financing in the province (Marchildon and Schrijvers 2011). Following mediation, a compromise was reached that enabled physicians to secure concessions around reimbursement and for the Saskatchewan Medical Care Insurance Act to move forward (Marchildon and Schrijvers 2011). Nurses in Canada – 90% of whom are unionized – have also engaged in multiple forms of resistance, including protests and strikes in multiple provinces over several decades, catalyzed by myriad concerns, including working conditions, compensation and labour rights (Briskin 2011). In 2004, the Hospital Employees' Union in British Columbia launched an unauthorized strike resisting privatization and contracting of food, housekeeping, laundry and other services to for-profit transnational companies (Isitt and Moroz 2007). In recent years, Canadian medical students have advocated for urgent attention to the climate crisis and other key social movements, such as Indigenous Peoples' rights and racial justice (Jane et al. 2022). These examples illustrate the important role of protest and strike action as platforms for the Canadian health workforce to express concerns and demand change in the absence of consistent and inclusive mechanisms for policy dialogue. However, it is important to recognize that health workers are heterogeneous, with considerable diversity in the workforce in terms of factors such as gender, race, country of origin and levels of unionization (CAHS 2023; Statistics Canada 2024), and hold diverse values and perspectives, resulting in varied drivers of protest and strike action that are in need of scholarly attention.
Health worker protests therefore provide a vital lens into the policy demands put forward by health workers and suggest important learnings for the influence of these groups on health policy processes. Despite the growing public attention to healthcare workers' protests, little scholarly attention has been paid to these forms of labour protests in interdisciplinary health scholarship (for exceptions, see Brophy et al. 2022; Russo et al. 2019; Trappman et al. 2022). In Canada, these dynamics are a crucial aspect of health workforce governance and health policy processes provincially and nationally, but it is yet to be investigated comprehensively. This paper begins to address this gap through a descriptive analysis of healthcare worker protests in Canada between January 2021 and December 2022 included within the ACLED project database. We focus on the following dimensions of health worker protests and strike action: (1) the quantity, clustering and distribution of protest and strike action in Canada; (2) policy demands expressed by organizers; and (3) the temporal sequence of protests in 2021 and 2022. We conclude with a discussion on the health workforce crisis as a policy issue arising, in part, from the culmination of these unmet demands.
Data and methodology
Data for this article come from the ACLED database (Raleigh et al. 2010), a comprehensive database of event-level information on protest action and political violence sourced from local, national and international media sources; non-governmental and governmental organizations' reports; and vetted social media. Events are defined as an occurrence involving designated actors, which occurs at a specific location on a specific day (ACLED 2024a: 9). Furthermore, ACLED defines a protest as “a public demonstration in which the participants do not engage in violence, though violence may be used against them” (ACLED 2024a: 13). For example, ACLED captures public protest rallies by health workers but does not capture non-public lobbying activities by advocacy groups (such as that described by Glynn 2023). Since ACLED specifies the actors involved in given events, we were able to isolate events involving health workers. ACLED defines health workers as “all civilians who engage in actions with the primary goal of providing health services to a community,” including doctors, nurses, long-term care workers, midwives and other health professions (ACLED 2024b). The reliability and validity of events included in ACLED is ensured by in-house data collection review, test intercoder reliability and methodological consistency (ACLED 2023a, 2023b).
We used a dataset from ACLED that captured all health worker-involved protest events in Canada between January 2021 and December 2022. Our data are limited to this time frame as ACLED only began coverage of Canada in 2021. We applied an existing protest event coding framework to classify the different types of health worker protest events in Canada (Brophy et al. 2022). This framework classifies the drivers of health worker protest events into five major categories: (1) resources (RES), (2) working conditions and remuneration (WCR), (3) health service delivery (HSD), (4) public policy (PUBPOL), and (5) other. RES refers broadly to material supplies needed for health workers to perform their duties, such as personal protective equipment (PPE). WCR captures protests regarding compensation, worker safety and other related concerns. HSD refers to issues within the health system more broadly and the ability of health workers to provide care within the system, including underfunding of healthcare, infrastructure and quality of care. PUBPOL includes other government programs and policies not explicitly related to healthcare delivery, such as stay-at-home orders and environmental concerns. The final category, other, captures the small number of protest drivers that do not readily fit into the other categories, such as protests of solidarity with other workers and demanding recognition for work. In addition, we included subcategories of each primary category to further illuminate the nuances of each protest event. For example, one of the subcategories under WCR is compensation, which includes delayed pay, unemployment pay, risk allowances and related concerns. A complete codebook is available as an online supplement.
The initial codebook was applied to a subset of protest events, with additional subcategories added to categorize protest demands that were not accurately captured in the existing codebook. The coding of protest events was conducted independently and in duplicate to ensure accuracy. One analyst was the primary coder and classified all protest events independently. Two other analysts each coded approximately 20% of the dataset independently to ensure accuracy. All discrepancies in coding were resolved through discussion within the team.
Data preparation and descriptive analyses were run in Microsoft Excel. We computed counts of protests in specific provinces, counts of specific types of protests and counts of protests according to categories in the codebook and created a timeline of protest count over time. In addition, we used Tableau to produce a map of health worker protest locations across Canada using the longitude and latitude coordinates provided in the ACLED database. Ethics approval was not required for this observational study of aggregated data.
Results
In total, our dataset includes 157 unique events. We categorized each event based on its method of protest (armed conflict, peaceful gathering, etc.) using the ACLED (2024a: 26–28). The majority of recorded protests (n = 151) were one-sided and peaceful events. Seven protests – all concerning anti–COVID-19 mitigation approaches – involved counter protesters. Five protests were categorized as two-sided peaceful events due to the presence of counter protesters, some of whom were identified as healthcare workers in support of public health measures. Two protests involving both protesters and counter protestors (the latter including healthcare workers) were a part of the 2022 Freedom Convoy and involved some element of police involvement in managing safety of attendees. While all events captured within our dataset are coded as a type of protest event, there was one event in Ontario that is described in the ACLED database as a strike and picket line.
Overall, there were 0.42 protest events per 100,000 population within Canada (Statistics Canada 2023). The province of Ontario saw the highest number of unique protest events, with 63 events captured within our time frame. Quebec and British Columbia saw the second-highest number of protest events, with 25 recorded in each province. Alberta recorded the next highest number of events with 18. The remaining provinces experienced six or fewer events over the same period, and there were no recorded protest events in the three territories. Of the 157 events captured in our database, 74 (47.1%) were identified as having union involvement, that is, any event within the database that identified a union or union members as participants or organizers of the event.
The timeline in Figure 1 outlines a temporal account of the number of unique protest events by date. While most datapoints indicate single-site events, a few clusters of protests occurred. By cluster event, we mean a group of more than one protest event that occurred on the same day that are connected through a shared organization and protest aim. The first cluster took place on September 1, 2021, as part of a “worldwide walk” (Worldwide Walkout for Health Freedom) and included 12 protests in four provinces led by the Canadian Frontline Nurses network, a group focused on advocacy against various COVID-19 mitigation strategies (vaccine mandates, mandatory masking, etc.) (CBC News 2023). The Canadian Frontline Nurses network was not affiliated with recognized labour unions and was, in fact, denounced by these same unions (CBC News 2021; Junker 2021). The second cluster that occurred on September 13, 2021, where protesters demonstrated against COVID-19 lockdowns in 13 cities across eight provinces (mostly concentrated in British Columbia but also in Alberta, New Brunswick, Ontario, Prince Edward Island, Quebec, Manitoba and Saskatchewan), was also organized by Canadian Frontline Nurses. Small groups of counter protesters supporting public health measures were present at multiple sites in this second cluster – Calgary, Edmonton, Saskatoon, Toronto and Winnipeg.
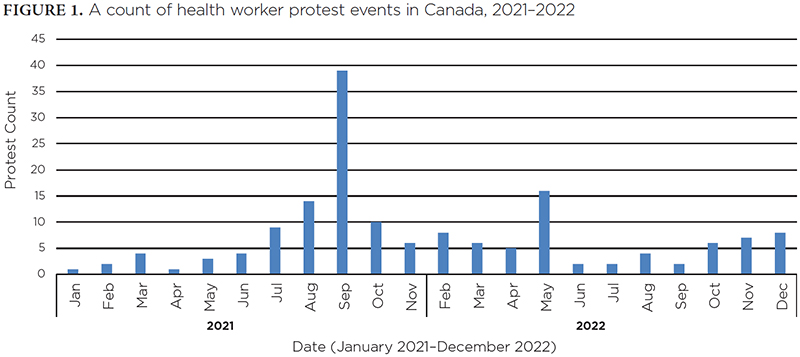
The final cluster occurred on December 12, 2022, across Ontario, where protesters demonstrated against the governing Conservative Party's handling of the health system crisis and the ongoing privatization of healthcare within the province, exacerbated by the introduction of Bill 124. This cluster of events was organized by the Ontario Health Coalition, a network of over 400 grassroots organizations in Ontario that supports progressive health policy and action. Some protest events in this cluster involved union members and leaders, particularly from the Canadian Union of Public Employees (CUPE).
Overall, WCR was the largest category with 91 protest events. HSD and PUBPOL also featured prominently, with 41 and 33 coded cases, respectively. Fewer cases were coded in the other category, numbering only seven cases total. There were no cases coded under the RES category. The number of primary categories exceeds the number of events due to select protest events focusing on more than one primary area of concern. For example, some protests were coded as both WCR and HSD, such as a motorcade protest organized by the United Nurses of Alberta on September 17, 2021, against understaffing (captured under HSD) and underfunding (captured under WCR). Protests involving unions focused on demands such as compensation (n = 31), contract negotiation (n = 7) and privatization (n = 7), while protests organized without explicit union presence or involvement included a dominant focus on anti-vaccination advocacy (n = 34), compensation (n = 16) and understaffing or patient overload (n = 6).
Figure 2 outlines the distribution of protest events by policy demand across Canada. The distribution of protest events appears to reflect provincial population densities, with most protest events occurring in Ontario, Quebec and British Columbia. However, the distribution of protest categories varies between provinces. For example, the majority of protest events in British Columbia focused on PUBPOL, while protests in Quebec were primarily concerned with WCR. One example of a remuneration-focused protest in Quebec occurred on February 11, 2021, when a small group of healthcare workers staged a protest outside of Quebec Premier Francois Legault's office to demand hazard pay during the COVID-19 pandemic and recognition of their work throughout the pandemic. Provincial variation may be indicative of contextual realities between the provinces during the period of analysis, such as the dispute over Bill 124 in Ontario, which prompted 11 protest events explicitly against the legislation.
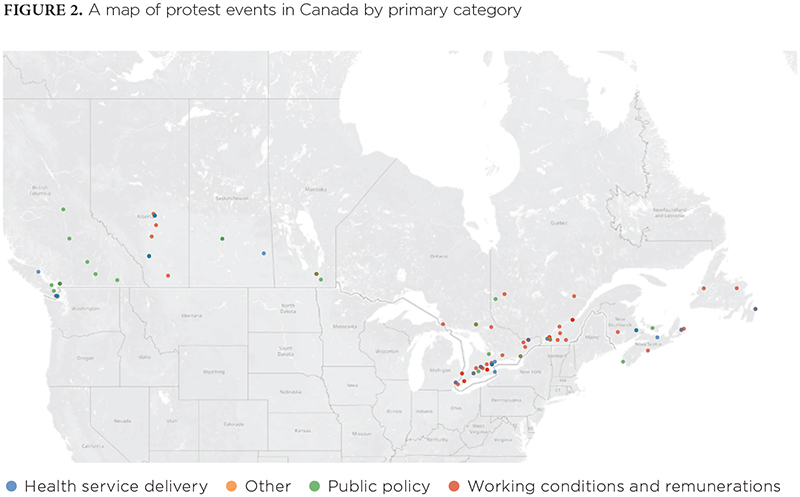
Table 1 examines our coding at the secondary category level, analyzing the specific area of focus for each protest event. Overall, compensation was the largest category of targeted issues within our cases, followed closely by vaccination. Notably, all vaccination-focused protests expressed anti-vaccine sentiment rather than demonstrating for increased vaccination rates, accessibility of vaccinations or other expressions of support for vaccination. Understaffing/patient overload, privatization, anti–COVID-19 mitigation strategies and union contracts/negotiations also occurred frequently within the dataset. There were eight protests concerning unspecified working conditions (i.e., the case description within the ACLED dataset did not specify which working conditions were being protested) and six expressing solidarity with other workers. The remaining issues were featured in less than five protest events each throughout the time frame included in this dataset. Similar to the primary level of coding, our total number of coded events exceeds 157 due to select cases focusing on multiple issues simultaneously. Table 2 displays data on healthcare worker populations by province. An analysis of event data by protest demands and provinces is available in Appendix 1, available online here.
| TABLE 1. Counts of primary and secondary protest demands | ||
| Main category of protest demand | Subcategory of protest demand | Count |
| WCR | Compensation | 48 |
| PUBPOL | Anti-vaccination | 38 |
| HSD | Understaffing/patient overload | 19 |
| HSD | Privatization | 13 |
| PUBPOL | Anti–COVID-19 mitigation strategies | 13 |
| WCR | Union contracts/negotiations | 11 |
| WCR | Working conditions | 8 |
| Other | Solidarity | 6 |
| HSD | Spending/underfunding | 4 |
| HSD | Quality of care/facilities/healthcare system | 4 |
| PUBPOL | Anti-masking policies | 3 |
| HSD | Health system capacity | 3 |
| Other | Recognition of work/sacrifice | 3 |
| HSD | Health infrastructure | 3 |
| PUBPOL | Mitigation strategies | 3 |
| All other subcategories (< = 2 counts each; e.g., provincial health coverage, health disparities, dismissal, violence toward health workers, job security, social and living supports, worker protections) | 19 | |
| HSD = health service delivery; PUBPOL = public policy; WCR = working conditions and remuneration. | ||
| TABLE 2. Provincial analysis of protest events | ||||
| Province | Number of health workers by CIHI definition (2017–2021 average) | Number of health workers per 100,000 population (2017–2021 average) | Number of protests | Protests per 1,000 health workers |
| Newfoundland and Labrador | 25,458 | 4,860 | 5 | 0.196 |
| Prince Edward Island | 7,078 | 4,498 | 1 | 0.141 |
| Nova Scotia | 46,088 | 4,749 | 6 | 0.130 |
| New Brunswick | 35,530 | 4,571 | 5 | 0.141 |
| Quebec | 335,119 | 3,953 | 25 | 0.075 |
| Ontario | 523,005 | 3,607 | 63 | 0.120 |
| Manitoba | 56,260 | 4,123 | 6 | 0.107 |
| Saskatchewan | 48,874 | 4,182 | 3 | 0.061 |
| Alberta | 185,859 | 4,270 | 18 | 0.097 |
| British Columbia | 180,239 | 3,547 | 25 | 0.139 |
| Yukon | 1,909 | 4,619 | 0 | N/A |
| Northwest Territories | 637 | 1,410 | 0 | N/A |
| Nunavut | 451 | 1,169 | 0 | N/A |
| CIHI = Canadian Institute for Health Information. | ||||
Discussion
This paper presents descriptive evidence regarding the scale and scope of protest action by health workers in Canada during 2021 and 2022. Events were reported in every province during the time period studied, though no events were captured in the Northwest Territories, Yukon or Nunavut. The highest absolute numbers of protest activity were seen in Ontario, with the Maritime provinces seeing the least protest activity during the period of analysis. Protest activity appears to follow population density trends, with the most populous provinces (Ontario, Quebec and British Columbia) seeing the most activity in terms of absolute numbers. Nearly half of all protests involved unions as participant organizers of the event (47.13%). Protest demands were heterogeneous. Overall, more than 57% of protests focused on WCR broadly understood, and compensation (n = 48) and understaffing/patient overload (n = 19) were the most frequently occurring secondary categories. Protests organized by unions were primarily concerned with remuneration, working conditions and healthcare systems as opposed to those organized by non-union organizations, which included a sizable focus on anti–COVID-19 mitigation measures, such as anti-vaccination (n = 38), other anti-mitigation measures (n = 13) and anti-masking policies (n = 3).
Existing research on protests and strike action by health workers in Canada has tended to focus on particular occupational groups or has applied a historical analysis of incidents from across Canada (Briskin 2012; Heron and Smith 2020). Our study contributes to this literature by providing a comprehensive measure of health worker protest activity in a two-year time period, capturing commonalities across protest demands and connections between protesting groups. The distinctive nature of contextual factors during this time period (2021–2022) resulted in a focus on protest demands that might not have otherwise emerged as salient, that is, COVID-19 mitigation measures. That said, external shocks such as COVID-19 are often the site of emergent social movements, serving as a window into issue identification and framing (Pleyers 2020). While the anti–COVID-19 mitigation protests were organized by a small number of individuals with explicit disapproval and denunciation from unions, emerging research is indicative of the social movement potential of anti-vaccine and COVID-19–denialist groups such as Canadian Frontline Nurses (Rohlinger and Meyer 2024; Wolf and Theunissen 2023; Zajak 2023). The potential harms of such advocacy – arguably more potent due to the involvement of health workers – are now readily apparent in rising vaccine hesitancy and mistrust of public health advice in Canada and globally. This finding provides an impetus for further research and analysis on the nature of healthcare workers' involvement in opposing public health measures. Practice implications could include the development of efforts to counter misinformation and periodic awareness building programs around public health programs, such as immunization campaigns, for the health workforce.
Our findings align with research on protest demands, which demonstrate the dominance of concerns regarding compensation and working conditions. A review of protests by health workers in the first year of the pandemic (March 2020 to March 2021) found that of the 6,589 protests by health workers in 149 countries, 66% concerned working conditions and compensation (Brophy et al. 2022). Research on health worker protests in 90 countries during the COVID-19 pandemic (Trappman et al. 2022) similarly found that the majority of protests concerned compensation, followed by PPE and safety concerns. Russo et al. (2019) similarly highlighted that prior to COVID-19, in low-income countries, many events were motivated by compensation and working conditions. Our study builds on previous research by highlighting the diverse concerns voiced by health workers in Canada, such as several protests regarding healthcare systems and reform (e.g., privatization).
Our research has identified key areas of concern for Canadian health workers, including compensation, working conditions and systemic challenges pertaining to healthcare access and quality. Engaging with the workforce and systems-level concerns expressed by health workers through dialogue and policy development provides a pathway for the federal and provincial governments to make sustainable progress toward addressing the health workforce crisis. There are growing concerns among the public regarding provincial health systems; a recent poll indicated that 86% of people surveyed are worried about the state of healthcare in their province (Canadian Press 2023). Failing to act on long-term policy concerns expressed by the health workforce may exacerbate the health workforce crisis, driving further discontent from health workers and the public.
Nearly half of the protest events examined here had union involvement, further strengthening the case for investigating health worker organizations as highly relevant policy stakeholders. In addition to expressing policy preferences, protests may also impact government policy directly; following mobilization by Ontario labour forces, the government repealed Bill 124 after a lengthy legal challenge (Casey and Jones 2024). Examples of protests and strikes shaping health policy in Canada are found throughout the trajectories of healthcare policy in Canada, most notably, the 1962 Saskatchewan doctors' strike (Marchildon and Schrijvers 2011). However, disentangling the precise causal relationship between protest activity and policy amendment, particularly given the context specificity of labour organizing across the provinces, requires further in-depth study.
Our results yield a few notable outcomes, which prompt questions for future research. First, a significant number of protest events focused on vaccine mandates, or COVID-19 mitigation more broadly. The descriptions of these protests in ACLED indicated that they were primarily negative in sentiment, protesting against rather than in favour of vaccines or other mitigation measures. Asymmetry in sentiments toward vaccinations and mitigation measures may also be due to pro-vaccination and pro–COVID-19 mitigation strategies with health worker coalitions being less likely to attend gatherings in person within the study period. Future research on the sentiment of the COVID-19 era healthcare worker protests could illuminate the stances of healthcare workers on COVID-19 mitigation measures across regions, countries and fields of practice. Second, certain unions organized multiple protest events, occurring over consecutive days and in different locations. Future in-depth research could examine such episodes in order to identify changing organizational practices and strategies over time. Third, our findings on the drivers of health worker protests suggest that further comparative research, within Canada and between Canada and other jurisdictions, will yield important insights regarding broader structural challenges in the health sector.
For example, while compensation was a secondary category identified in this study, it may help to investigate geographic differences in protest distribution with this demand across provinces. An inter-provincial examination of health worker protests in Canada may illuminate key differences or similarities between provinces' experiences with these protest events, such as their thematic focus, strategies and catalysts for mobilization. Furthermore, the Canadian case reflects previous international findings, which indicate that health worker protests during the COVID-19 pandemic have predominantly focused on compensation and working conditions. This similarity prompts the opportunity to explore the impact of large-scale catalysts on health workers' demands during protests and strikes, and whether such events present differently in various contexts. Lastly, some provinces have legislation, which prevents certain sectors from engaging in legal strikes. In Ontario, nurses do not have the right to strike as per the Hospital Labour Disputes Arbitration Act (CanLII 1990). A deeper exploration into the relationship between anti-strike legislation and protest and strike activity may yield important insights into labour mobilization (or non-mobilization) to express policy preferences.
Limitations
There are certain limitations to our study that must be considered in interpreting the results. First, while the ACLED database is the most comprehensive available source for identifying health worker protests, it is possible that certain events were not captured by their data collection methods. ACLED acquires data from four sources: traditional media, reports, local partner data and new forms of media (e.g., WhatsApp). Traditional media includes “all subnational, national, regional, and international media outlets that are governed by journalistic principles of verification” (ACLED 2023c, p. 2). A protest event that received no media coverage would not be included within the ACLED database and would be subsequently uncaptured by our coding. Because information about protest actors is sourced from media as opposed to surveys, important attributes such as identity demographics, wage levels of protesters and accurate standardized estimates of protest sizes are not included in the database. Union and organized participation were typically mentioned in media sources, and thus, we could further examine them in our coded dataset. We are unaware of linkable sources for other potential variables of interest, which should be the focus of future work in this area. Second, the ACLED definition of health workers includes a broad range of occupations; however, certain occupational groups in the health sector that are not more directly engaged in various aspects of HSD, such as planners or decision makers, might have been omitted from data collection and therefore are not included in this analysis. Third, we deduced the motivating forces for protest events from short summaries included in the ACLED database, and therefore, additional protest categories might not have been identified. Finally, protests must be seen as only one vehicle for expressing policy demands; future research may examine how protest aligns with policy preferences of health workers and overall policy agendas of organizations representing health workers.
Conclusion
Policy preferences of health workers are an important influence on health policy, and public policy more broadly. The role of health worker protests and strikes in shaping these processes is underexamined within the public health literature. Many of the policy preferences expressed by health workers in our study reflect issues that underpin the ongoing health workforce crisis, a major policy issue. Our research addresses part of this gap by examining Canadian health worker protests during the COVID-19 pandemic to identify spatial and thematic trends in protest activity. Our results indicate thematic similarities between Canada and international jurisdictions, wherein health worker protests have predominantly focused on compensation and other working conditions. However, protest demands were also diverse, including protests against COVID-19 mitigation strategies and protests supporting health system reform. Addressing the health workforce crisis will require continued engagement with health workers as stakeholders and the recognition that protest demands can help identify solutions to the workforce crisis. Future comparative studies of health worker protests may further illuminate the causes and strategies of these protest events, analyzing both inter- and intra-national cases. Furthermore, additional examinations of health worker protests and their sentiment regarding COVID-19 mitigation may yield insight into variations between regions, countries and medical professions. It is unclear how protest activity will evolve in future years, prompting the opportunity for longitudinal research on health worker protests.
Correspondence may be directed to Veena Sriram by e-mail at veena.sriram@ubc.ca.
Manifestations des travailleurs de la santé au Canada: analyse descriptive des événements de protestation en 2021 et 2022
Résumé
Objectif: Nous avons analysé les mouvements de protestation organisés par des travailleurs de la santé au Canada en 2021 et 2022. Notre analyse s'est concentrée sur la quantité et la répartition des manifestations au Canada, sur les revendications politiques exprimées par les organisateurs et sur la séquence temporelle des manifestations.
Méthode: Nos données proviennent du projet ACLED (Armed Conflict Location and Event Data), qui comprend un ensemble de données sur tous les événements de protestation qui impliquent des travailleurs de la santé dans certains États, dont le Canada. Au moyen d'une taxonomie déjà en place sur les revendications politiques, nous avons analysé des types précis de manifestations, de revendications et de tendances temporelles.
Résultats: Pour la période visée par notre étude, l'ACLED recense 157 manifestations de travailleurs de la santé. Toutes les provinces ont connu ce type de manifestations, l'Ontario ayant enregistré la plus forte proportion (~40 %). La majorité des manifestations portaient sur les conditions de travail et la rémunération (57 %), suivies par les politiques publiques (26 %) et la prestation des services de santé (21 %). Les sous-catégories les plus fréquentes étaient la rémunération (n = 48), l'opposition aux obligations vaccinales (n = 38) et le manque de personnel ou la surcharge des patients (n = 19).
Conclusion: Les travailleurs de la santé au Canada font état de préoccupations en matière de politique publique, préoccupations qui vont de l'opposition aux mesures d'atténuation de la COVID-19 au sous-investissement dans les systèmes de santé. L'identification et la reconnaissance de ces facteurs, ainsi que l'élaboration d'une politique ciblée pour y faire face grâce à un engagement inclusif et soutenu auprès des travailleurs de la santé, contribueront à trouver des solutions à long terme.
About the Author(s)
Veena Sriram, MPH, Phd, School of Population and Public Health, School of Public Policy and Global Affairs, University of British Columbia Vancouver, BC
Meena Rakasi, BA, University of Chicago Chicago, IL, US
Kartik Sharma, BA, MSC, Centre for Health Services and Policy Research, University of British Columbia Vancouver, BC
Michael R. Law, Phd, Centre for Health Services and Policy Research, School of Population and Public Health, University of British Columbia Vancouver, BC
Sorcha A. Brophy, Phd, Mailman School of Public Health, Columbia University New York, NY, US
Acknowledgment
We thank Katelynn Kowalchuk for their contributions to the project.
References
Armed Conflict Location and Event Data (ACLED). 2023a, March. Quick Guide to ACLED Data. Retrieved August 15, 2023. <https://acleddata.com/resources/quick-guide-to-acled-data/#s13>.
Armed Conflict Location and Event Data (ACLED), 2023b, March 1. How Does ACLED Code and Review Data to Ensure Quality? Retrieved August 15, 2023. <https://acleddata.com/knowledge-base/how-does-acled-code-and-review-data-to-ensure-quality/>.
Armed Conflict Location and Event Data (ACLED). 2023c, March. FAQs: ACLED Sourcing Methodology. Retrieved August 15 2012. <https://acleddata.com/acleddatanew/wp-content/uploads/dlm_uploads/2023/03/FAQs_ACLED-Sourcing-Methodology.pdf>.
Armed Conflict Location and Event Data (ACLED). 2024a, October 3. Armed Conflict Location & Event Data Project (ACLED) Codebook. Retrieved December 1, 2024. <https://acleddata.com/acleddatanew/wp-content/uploads/2021/11/ACLED_Codebook_v1_January-2021.pdf>.
Armed Conflict Location and Event Data (ACLED). 2024b, May 7. Health Workers: Scope and Coverage in ACLED Data. Retrieved December 1, 2024. <https://acleddata.com/knowledge-base/faqs-disorder-involving-health-workers/>.
Ahmed, A., F. Chouairi and X. Li. 2022. Analysis of Reported Voting Behaviors of US Physicians, 2000–2020. JAMA Network Open 5(1): e2142527. doi:10.1001/jamanetworkopen.2021.42527.
Berkhout, S.G., K.A. Sheehan and S.E. Abbey. 2021. Individual and Institutional-Level Concerns of Health Care Workers in Canada During the COVID-19 Pandemic. A Qualitative Analysis. JAMA Network Open 4(7): e2118425. doi:10.1001/jamanetworkopen.2021.18425.
Bonica, A., H. Rosenthal and D.J. Rothman. 2014. The Political Polarization of Physicians in the United States: An Analysis of Campaign Contributions to Federal Elections, 1991 Through 2012. JAMA Internal Medicine 174(8): 1308–17. doi:10.1001/jamainternmed.2014.2105.
Brewster, M. and V. Kapelos. 2020, May 26. Military Alleges Horrific Conditions, Abuse in Pandemic-Hit Ontario Nursing Homes. CBC News. Retrieved April 10, 2025. <https://www.cbc.ca/news/politics/long-term-care-pandemic-covid-coronavirus-trudeau-1.5584960>.
Briskin, L. 2012. Resistance, Mobilization and Militancy: Nurses on Strike. Nursing Inquiry 19(4): 285–96. doi:10.1111/j.1440-1800.2011.00585.x.
Brophy, S.A. and V. Sriram. 2021, August 1. Introduction to “Recontextualizing Physician Associations: Revisiting Context, Scope, Methodology”. J Health Polit Policy Law; 46(4): 641–52. doi.org/10.1215/03616878-8970852.
Brophy, S.A., V. Sriram, H. Zong, C. Andres, M.P. Mawyin and G.L. Narayanan. 2022, April. Heroes on Strike: Trends in Global Health Worker Protests During COVID-19. Accountability Research Center. Retrieved August 1 2023. <https://accountabilityresearch.org/wp-content/uploads/2022/04/ARC-Accountability-Note_Health-Worker-Protests_WEB.pdf>.
Canadian Academy of Health Sciences (CAHS). 2023, March. Canada's Health Workforce: Pathways Forward. An Assessment by the Canadian Academy of Health Sciences. Retrieved October 10, 2023. <https://cahs-acss.ca/wp-content/uploads/2023/04/CAHS-Health-Workforce-Pathways-Forward-EN_Final_Apr-4.pdf>.
CanLII. 1990. Hospital Labour Disputes Arbitration Act, RSO 1990, c. H.14. Retrieved October 1, 2023. <https://www.canlii.org/en/on/laws/stat/rso-1990-c-h14/latest/rso-1990-c-h14.html#document>.
Casey, L. and A. Jones. 2024, February 12. Ontario to Repeal Wage-Cap Law After Appeal Court Rules Ford Government's Bill 124 Unconstitutional. CBC News. Retrieved December 1, 2024. <https://www.cbc.ca/news/canada/toronto/bill-124-appeal-court-ruling-ontario-1.7112291>.
CBC News. 2023, September 1. Reports of Assault, Verbal Abuse as Thousands Protest Vaccine Passports Outside Hospitals Across B.C. Retrieved December 1, 2023. <https://www.cbc.ca/news/canada/british-columbia/vaccine-passport-protest-1.6161817>.
CBC News. 2021, September 13. Nurses Denounce Anti-Vaccine Passport Protest in St. John's. CBC News. Retrieved December 1, 2023. <https://amp.cbc.ca/news/canada/newfoundland-labrador/anti-vaccination-passport-protest-st-johns-1.6173996>.
Drummond, D., D. Sinclair and J. Gratton. 2022, November 2. Troubles in Canada's Health Workforce: The Why, the Where, and the Way Out of Shortages. C.D. Howe Institute. Retrieved August 1, 2023. <https://cdhowe.org/publication/troubles-canadas-health-workforce-why-where-and-way-out-shortages/>.
Duong, D. and L. Vogel. 2023, February 27. Overworked Health Workers Are “Past the Point of Exhaustion.” CMAJ 195: E309–10. doi:10.1503/cmaj.1096042.
Gajjar, J., N. Pullen, Y. Li, S. Weir and J.G. Wright. 2022. Impact of the COVID-19 Pandemic Upon Self-Reported Physician Burnout in Ontario, Canada: Evidence From a Repeated Cross-Sectional Survey. BMJ Open 12(9): e060138. doi:10.1136/bmjopen-2021-060138.
Glynn, T. 2023, December 10. Health & Hope Lobby on Parliament Hill. Canadian Health Coalition. Retrieved December 1, 2024. <https://www.healthcoalition.ca/registration-opens-for-health-hope-lobby-on-the-hill/>.
Government of Canada. 2023, June 28. Canada Announces New Immigration Stream Specific to Health Workers. Retrieved December 1, 2023. <https://www.canada.ca/en/immigration-refugees-citizenship/news/2023/06/canada-announces-new-immigration-stream-specific-to-health-workers.html>.
Grant, K. 2023, July 24. Ontario Spending on Private Nursing Agencies Quadrupled Since COVID-19, Data Show. The Globe and Mail. Retrieved December 1, 2023. <https://www.theglobeandmail.com/canada/article-ontario-hospitals-private-nurses/>.
Hagedorn, J., C.A. Paras, H. Greenwich and A. Hagopian. 2016. The Role of Labor Unions in Creating Working Conditions That Promote Public Health. American Journal of Public Health 106(6): 989–95. doi:10.2105/AJPH.2016.303138.
Heron, C. and C. Smith. 2020. The Canadian Labour Movement: A Short History (4th edition). Lorimer. Retrieved December 1, 2023. <http://www.lorimer.ca/adults/Book/3141/The-Canadian-Labour-Movement.html>.
Isitt, B. and M. Moroz. 2007. The Hospital Employees' Union Strike and the Privatization of Medicare in British Columbia, Canada. International Labor and Working-Class History 71: 91–111. doi:10.1017/S014754790700035X.
Jane, A., G. Forster and C. Faulkner. 2022. Canadian Medical Student Climate Advocacy During the COVID-19 Pandemic. The Lancet Planetary Health 6(3): E186–87. doi:10.1016/S2542-5196(22)00011-0.
Jena, A.B., A.R. Olenski, D. Khullar, A. Bonica and H. Rosenthal. 2018. Physicians' Political Preferences and the Delivery of End of Life Care in the United States: Retrospective Observational Study. The BMJ 361: k1161. doi:10.1136/bmj.k1161.
Jones, A. 2019, November 8. Ontario Passes Bill to Cap Public Sector Wage Increases at One Per Cent. CTV News. Retrieved December 1, 2023. <https://toronto.ctvnews.ca/ontario-passes-bill-to-cap-public-sector-wage-increases-at-one-per-cent-1.4675970>.
Junker, A. 2021, September 13. Alberta Government, AHS Condemn Anti-Vaccine Protests at Alberta Hospitals. Edmonton Journal. Retrieved December 1, 2023 <https://edmontonjournal.com/news/local-news/justice-minister-condemns-planned-anti-vaccine-protests-at-alberta-hospitals>.
Kalifa, A., A. Okuori, O. Kamdem, D. Abatan, S. Yahya and A. Brown. 2022. “This Shouldn't Be Our Job to Help You Do This”: Exploring the Responses of Medical Schools Across Canada to Address Anti-Black Racism in 2020. CMAJ 194(41): E1395–403. doi:10.1503/cmaj.211746.
Lasco, G., R.M. Yunus, E.C. Dee and M. McKee. 2022. Health Workers on the Political Frontlines. Health and Human Rights Journal 24(1): 121–23.
Laugesen, M.J. 2019. How the American Medical Association's Rent-Seeking Strategy Compensated for Its Loss of Members. Journal of Health Politics, Policy and Law 44(1): 67–85. doi:10.1215/03616878-7206731.
Leo, C.G., S. Sabina, M.R. Tumolo, A. Bodini, G. Ponzini, E. Sabato et al. 2021. Burnout Among Healthcare Workers in the COVID-19 Era: A Review of the Existing Literature. Frontiers in Public Health 9: 75029. doi:10.3389/fpubh.2021.750529.
Marchildon, G.P. and K. Schrijvers. 2011. Physician Resistance and the Forging of Public Healthcare: A Comparative Analysis of the Doctors' Strikes in Canada and Belgium in the 1960s. Medical History 55(2): 203–22. doi:10.1017/s0025727300005767.
Mavis Mulaudzi, F., M. Mulaudzi, R.A. Anokwuru and M. Davhana-Maselesele. 2021. Between a Rock and a Hard Place: Ethics, Nurses' Safety, and the Right to Protest During the COVID-19 Pandemic. International Nursing Review 68(3): 270–78. doi:10.1111/inr.12703.
Pleyers, G. 2020. The Pandemic Is a Battlefield: Social Movements in the COVID-19 Lockdown. Journal of Civil Society 16(4): 295–312. doi:10.1080/17448689.2020.1794398.
Raleigh, C., R. Linke, H. Hegre and J. Karlsen. 2010. Introducing ACLED: An Armed Conflict Location and Event Dataset. Journal of Peace Research 47(5): 651–60. doi:10.1177/0022343310378914.
Rohlinger, D.A. and D.S. Meyer. 2024. Protest During a Pandemic: How COVID-19 Affected Social Movements in the United States. American Behavioral Scientist 68(6): 810–28. doi:10.1177/00027642221132179.
Russo, G., L. Xu, M. McIsaac, M.D. Matsika-Claquin, I. Dhillon, B. McPake et al. 2019. Health Workers' Strikes in Low-Income Countries: The Available Evidence. Bulletin of the World Health Organization 97(7): 460–67. doi:10.2471/BLT.18.225755.
Sriram, V., S.A. Brophy, K. Sharma, M.A. Elias and A. Mishra. 2023. Associations, Unions and Everything in Between: Contextualizing the Role of Representative Health Worker Organisations in Policy. BMJ Global Health 8(29): e012661. doi:10.1136/bmjgh-2023-012661.
Statistics Canada. 2023. Census Profile, 2021 Census of Population. Retrieved November 15, 2023. <https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/index.cfm?Lang=E>.
Statistics Canada. 2024. Union Status by Industry. Retrieved December 1, 2024. <https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410013201>.
Stewart, A. 2022, January 6. Canada Headed for Nursing Shortage “Beyond Anything We've Ever Experienced”: Experts. Global News. Retrieved November 15, 2023. <https://globalnews.ca/news/8487144/canada-covid-nursing-shortage-alarm/>.
Tasker, J.P. 2023, June 28. As Canada Grapples With a Doctor Shortage, Ottawa Announces Immigration Stream for Health Workers. CBC News. Retrieved November 15, 2023. <https://www.cbc.ca/news/politics/canada-doctor-shortage-immigration-1.6891603>.
The Canadian Press. 2023, January 27. Canadians Worried About the State of Provincial Health Systems: Poll. CTV News. Retrieved December 1, 2023. <https://www.ctvnews.ca/health/canadians-worried-about-the-state-of-provincial-health-systems-poll-1.6248713>.
Trappman, V., C. Umney, D. Neumann, M. Stuart, S. Joyce and I. Bessa. 2022. Labour Protests During the Pandemic: The Case of Hospital and Retail Workers in 90 Countries. International Labour Organization Working Paper 83. Retrieved November 15, 2023. <https://www.ilo.org/legacy/english/intserv/working-papers/wp083/index.html#ID0EZC>.
Wilson, K. 2022, November 29. Ford Government to Appeal Court's Decision to Strike Down Bill 124. CP24. Retrieved November 15, 2023. <https://www.cp24.com/news/2022/11/29/ford-government-to-appeal-courts-decision-to-strike-down-bill-124/>.
Wolf, K. and P. Theunissen. 2023. One Voice or Multi-Issue Movement? Exploring the Role of Bonding and Bridging Social Capital Within the COVID-19 Antivax Movement. Public Relations Review 49: 102316. doi:10.1016/j.pubrev.2023.102316.
World Health Organization (WHO). n.d. Health Workforce. Retrieved November 15, 2023. <https://www.who.int/health-topics/health-workforce#tab=tab_1>.
World Health Organization (WHO). 2019. Classifying Health Workers: Mapping Occupations to the International Standard Classification. Retrieved November 15, 2023. <https://cdn.who.int/media/docs/default-source/health-workforce/dek/classifying-health-workers.pdf?sfvrsn=7b7a472d_3&download=true>.
World Health Organization (WHO). 2023. WHO Health Workforce Support and Safeguards List 2023. Retrieved December 1, 2023. <https://iris.who.int/bitstream/handle/10665/366398/9789240069787-eng.pdf?sequence=1>.
Zajak, S. 2023. COVID-19 and the Reconfiguration of the Social Movements Landscape. In B. Breno and G. Pleyers, eds., Social Movements and Politics During COVID-19: Crisis, Solidarity and Change in a Global Pandemic (pp. 134–40). Bristol University Press.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed