
Healthcare Quarterly
Integrating Geriatric Teams in Primary Care: Transforming Aging Care Through Collaborative Models in Ontario
Abstract
Care models integrating geriatrics into primary care are emerging across Ontario. Referred to as Primary Care Integrated Geriatric Teams (PCIGTs), their evidence-based approaches improve access to specialized care and support for older adults. Seven Ontario models were highlighted through webinars held in spring 2025, attended by nearly 200 participants. Presenters and participants identified promising design features, key learnings and supports needed to advance goal-aligned care for older adults. Relevant to primary care transformation, health system redesign and policy efforts in Ontario and beyond, PCIGTs can support primary care attachment, reduce pressure on acute services and promote aging in place.
Introduction
In 2025, Ontario's Government announced the Primary Care Action Plan, aiming to attach 100% of Ontarians to primary care teams (PCTs) (Ministry of Health 2025). This goal is dependent on team-based models along with embedded specialists. The integration of specialized geriatric expertise is particularly critical for older adults, with an estimated 776,000 Ontarians aged 65 years and older living with frailty (PGLO 2026), more than 330,000 living with dementia (Alzheimer Society of Ontario 2025) and more than 27,000 older adults experiencing serious mental illness (Warren et al. 2023). Primary care, as currently structured, experiences challenges supporting the comprehensive assessment and interventions required to manage the complexity of these populations (de Levante Raphael 2022; Pham et al. 2025), who are also high users of health services and require frequent visits. Embedding geriatric expertise within primary care enables comprehensive assessment, interprofessional collaboration and the development and implementation of personalized care plans and creates capacity for improved care quality while increasing primary care attachment.
Models integrating specialized geriatric services (SGSs) into PCTs already exist. Early experiences suggest these models focus on the delivery of a multidimensional, comprehensive geriatric assessment (CGA) and tailored interventions. A CGA is considered the standard of care for older adults experiencing complex health conditions (e.g., dementia, frailty) and is a multi-domain, interdisciplinary process used to evaluate and respond to the biopsychosocial needs of older adults (Aggarwal et al. 2023; Dimitriadou et al. 2025). A recent review identified that high-quality interprofessional CGAs (e.g., conducted with interprofessional team members as well as physicians) supported comprehensive patient care, improved care coordination, enhanced diagnostic accuracy and increased patient and provider satisfaction (Nalla and Ehsan 2025). CGA delivered in primary care can help enhance access to specialized care and can build capacity in primary care for the ongoing care of complex older patients and their care partners.
In spring 2025, Provincial Geriatrics Leadership Ontario (PGLO) and the Regional Geriatric Program of Southwestern Ontario, entities coordinating geriatric services, provincially and regionally, held two webinars showcasing models referred to as Primary Care Integrated Geriatric Teams (PCIGTs) and later mapped common features against known design elements of integrated care for older adults living with complex health conditions (Horgan et al. 2020). From real-time feedback provided during the sessions by participants (n = 199) via Slido (slido.com), inductive thematic analysis was used to identify key audience themes and the supports required to advance the care of older adults in primary care settings. Our findings are relevant to decision-makers across multiple settings as well as policy makers.
Promising Practices
An overview of seven models of PCIGTs is presented in Table 1, available online here. Full recordings, presentation slides and presenter biographies are also available at https://geriatricsontario.ca/resources/presentations-and-resources-models-and-examples-of-primary-care-integrated-geriatric-teams-resources/.
Alignment of Model Features With Design Elements of Integrated Care for Older Adults
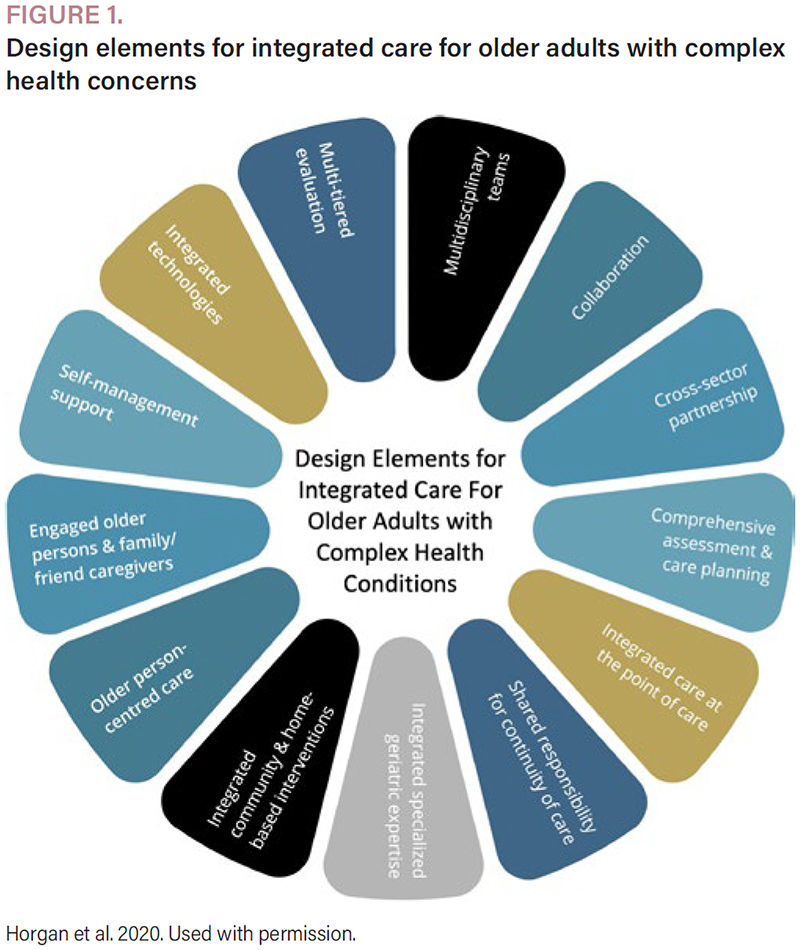
PGLO has previously identified 13 design elements for integrated care for older adults living with complex and chronic health needs (Figure 1).
{kind=link}

These design elements describe key evidence-based features that offer the most promise for holistic, patient-centred care and provide a helpful framework to examine integrated models of geriatric services and primary care. While we did not formally evaluate the models described, we conducted preliminary mapping of key features noted across the seven models against these design elements to highlight commonalities and inform future service design and evaluation.
Multidisciplinary/interprofessional teams
All models described interprofessional team members and care of the elderly (COE) physicians, geriatricians and, in some cases, geriatric psychiatrists working collaboratively with primary care providers (PCPs). The composition of these interprofessional teams varied across the province, typically combining existing primary care and SGS staff, supplemented by in-kind staff contributions from community partners. All models included team members with specific training in the care of older adults. In teams that had access to new funding, targeted staffing investments were made to address priority needs.
Collaboration
Central to these models was collaboration among internal and external team members practising to their full scope. Their efforts coordinated patient care, streamlined processes and reduced duplication of services. The degree of collaboration varied from cooperation to integration (Weaver 2021) and opened up an area for further study to identify optimal approaches.
Cross-sector partnership
While all teams identified roles for partners across multiple organizations, these arrangements varied from ad-hoc to formalized partnership agreements outlining specific accountabilities (e.g., sharing of staff, common reporting). Arrangements with some host organizations, usually Family Health Teams or Community Health Centres, included clinical space, administrative support and interprofessional team members to support itinerant geriatric specialists working on site during scheduled clinics. Many supports were provided in-kind, introducing precariousness into models if organizational pressures require hosts to redirect these supports. Mechanisms for ongoing funding across models were identified as a requirement for sustainability.
Comprehensive assessment and care planning
A key feature of most models was providing community access to CGA. It should be noted that where only one interprofessional team member (e.g., a registered nurse) completed a multi-domain assessment of the older adult, the term “geriatric assessment” was preferred.
In most PCIGT models, teams completed the CGA or geriatric assessment and followed up on recommendations generated. This direct support for follow-up overcame previously identified challenges by PCPs related to actioning recommendations arising from a CGA.
Integrated care at the point of care
In these seven models, health professionals of different disciplines who were knowledgeable in geriatrics worked within primary care settings to deliver care. Most models incorporated interdisciplinary rounds (usually weekly), which provided a venue to discuss and plan integrated patient care. Rounds also supported the PCT's capacity to provide ongoing care for older adults by incorporating topical learning sessions for the whole team.
Shared responsibility for continuity of care
While some models functioned in a consultative fashion (e.g., limited follow-up appointments), most provided ongoing support either directly to patients or indirectly by being available for consultation by the PCP. We did not identify which modalities were most effective under what circumstances, presenting an opportunity for further study. In addition, the delivery of geriatric care services within the context of the primary care medical “home” preserved continuity by allowing for ongoing collaboration between specialized providers and PCPs. Communication was facilitated through the use of the primary care site's electronic medical record (EMR) for documentation in most models, and through simple mechanisms (e.g., messaging features, telephone calls and conversations during rounds). Models that did not have access to the primary care EMR suggested this as an important area for improvement and better coordination.
Integrated specialized geriatric expertise
All models included direct access (either on-site or through telecommunication) to SGSs. Specialized geriatric expertise included physician specialists (e.g., geriatricians, geriatric psychiatrists), COE physicians (family physicians certified in care of the elderly) and interprofessional team members with training and experience in the care of older adults, who frequently acted as geriatric assessors. The SGS clinicians were usually part of a broader system of SGSs and connected to regional leadership and additional clinical expertise, usually through Regional Geriatric Programs or Departments of Geriatric Medicine. These regional connections provided education, training and implementation expertise and facilitated access to additional specialized care, enabling critical support for embedded clinicians and PCPs.
Several models also highlighted integration among different types of geriatric speciality care, such as the inclusion of geriatric psychiatry. This type of integration simplified access for patients requiring care across a continuum of geriatric specialties. As one participant noted, “geriatrics includes geriatric psychiatry” (webinar participant, personal communication, May 8, 2026).
Integrated community and home-based interventions
Most models described the capacity to carry out home visits and fostered linkages with community service providers and home care agencies. Presenters noted that models serving older adults with increasing frailty required home visit capability, as these patients may be unable to attend clinic appointments. Home-based CGA for older adults can decrease healthcare system costs and avoid hospitalization (Singh et al. 2022). Fostering closer relationships with home care agencies was also noted as an opportunity for the continued development of PCIGT models.
Older person-centred care
All models highlighted the benefit of integrated geriatric teams that can focus specifically on the needs of older adults, and many drew inspiration from the 5M's model of geriatric care (mind, medications, multi-morbidity, mobility and matters most) (Molnar and Frank 2019). Although goal-based care planning approaches were not explicitly discussed, a CGA relies on eliciting the goals of patients and care partners to inform and tailor treatment plans. Approaches to goal-based care planning could be further explored in future evaluations of PCIGT models.
Engaged older persons and caregivers
All models described clinical practices that engaged the older adult and their care partners in assessments, interventions (e.g., carrying out mobility exercises) and care conversations. One model also described the involvement of older adults and care partners in the design of the model itself.
Self-management support
All models described approaches that include interventions to maintain independence and autonomy. Among older adults living with dementia, frailty or mental health conditions, self-management frequently required consideration of cognitive function and the interplay of chronic diseases, as well as the involvement of supportive care partners, where present.
Integrated technologies
In most cases, PCIGTs leveraged local digital infrastructure. This included documenting directly in the EMRs of the hosting primary care practice, facilitated by local EMR-related privacy agreements rather than formalized data sharing agreements. Integrating new technologies is an area of ongoing development in the care of older adults and may include remote monitoring and artificial intelligence-enabled tools.
Multi-tiered evaluations
Most evaluative activities were localized to each specific model, and, at present, there are no common metrics collected across PCIGTs. A robust quality assurance system and the identification and collection of common metrics would improve understanding of the impact of PCIGT models and are essential for optimizing the spread of these promising practices. Evaluations could focus on the successful identification of older adults with complex needs and, as demonstrated through a recent study, the impact of PCIGTs on overall primary care visits, prescribing/deprescribing, and emergency department visits or avoidance (Heckman et al. 2025) or other outcomes.
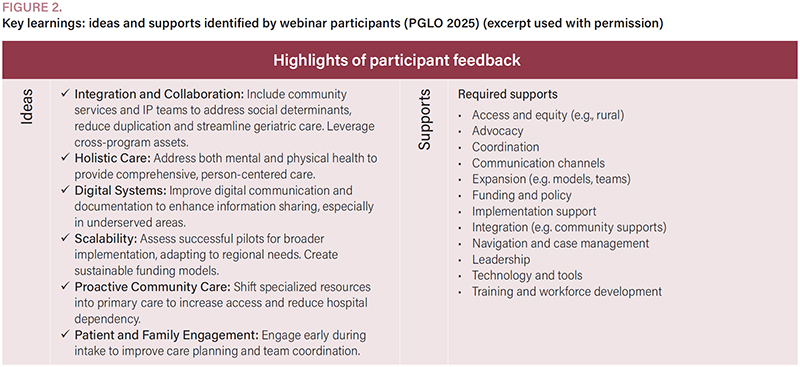
Webinar Participant Responses – What We Heard
During the webinars, we asked participants (n = 199), including at least 40 participants from PCT settings, to share ideas and identify supports required by their teams to advance the care of older adults in primary care settings. Figure 2 is an excerpt of a short report summarizing these key learnings found at https://geriatricsontario.ca/resources/presentations-and-resources-models-and-examples-of-primary-care-integrated-geriatric-teams-resources/.
{kind=link}

We also asked webinar participants to identify other attributes that resonated with them about the models presented. Themes identified included flexibility and variety; integration and collaboration; efficiency and workflow; access and outreach; funding and scalability; and tangible impact on outcomes. A detailed summary of additional participant responses is included in Table 2.
| TABLE 2. Key themes identified by webinar participants (n = 199) | |
| Question | Key themes |
| What resonated with you from the examples shared at today's webinar? | Flexibility and variety
|
| What supports do you and your team, or your local primary care colleagues, need to advance care of older adults in primary care settings? |
|
| COE = care of the elderly; EMR = electronic medical record. | |
Conclusion
Our webinars highlighted examples of localized work underway to support primary care's efforts to care for an aging population. Recognizing the provincial goal of supporting enhanced attachment to primary care, this paper provides key examples and identifies the components of successful models that can support the attachment and care of older adults living with complexity and their care partners. While most models demonstrated alignment with published design elements of integrated care for older adults living with complex health conditions, this paper also provides additional insights into areas that could be further refined, scaled and spread. In addition, there are opportunities for primary care to strengthen connections to Regional Geriatric Programs and the provincial network of geriatric services to garner critical support for emerging primary care-based models.
Future directions could include a focus on training, sustainable funding mechanisms, and technology and implementation supports. Emerging PCIGT models may provide new community training opportunities for interprofessional team members and medical residents, furthering an important shift to community-based models of geriatric care. Funding solutions may include the creation of alternate funding plans aligned to Primary Care Networks to foster recruitment of COE physicians and geriatric specialists, enabling reliable, accessible support for primary care, along with other funding packages to support these largely grassroots efforts. Technology and implementation supports can build on ideas presented in this paper, as well as future co-design and evaluation activities that could shape system transformation to address persistent wait times for SGSs and bolster primary care capacity for older adult care. Work underway to build PCIGT models informs future requirements for core clinical services focused on older adults living with complex health conditions and can ensure the availability of needed supports for aging in place in Ontario.
About the Author(s)
Kelly Kay, Phd, is the executive director at Provincial Geriatrics Leadership Ontario (PGLO), an entity that coordinates geriatric services across Ontario. Kelly is based in Toronto, ON and can be reached by e-mail at kelly.kay@geriatricsontario.ca.
Katie Bingham, MD, FRCPC, is a geriatric psychiatrist and clinician researcher with Waypoint Centre for Mental Health Care, Penetanguishene, ON, and a physician lead with North Simcoe Muskoka Specialized Geriatric Services, in Barrie ON.
Melanie Briscoe, OT Reg. (Ont.), MScOT, is the administrative director of the North East Specialized Geriatric Centre, based in Sudbury, ON, overseeing the Regional Geriatric Program of Northeastern Ontario and the continuum of Specialized Geriatric Services, with extensive experience leading innovative, system-level geriatric care across the region.
Cailin Campbell, MD, CCFP (COE), is a care of the elderly physician working at Brant Community Healthcare System and Grand River Community Health Centre, in Brantford, ON.
Sandra Easson-Bruno, MN, is from the Waypoint Centre for Mental Health Care. Sandra is the director of the North Simcoe Muskoka Specialized Geriatric Services program, a regional integrated specialized geriatric services program operating in Barrie, ON.
Jacobi Elliott, Phd, is a director with the Regional Geriatric Program of Southwestern Ontario, at St. Joseph's Health Care London, and a scientist with Lawson Research Institute. She works in London, ON.
Nicole Gallagher, PT, BScPT, serves as the regional clinical quality lead with North East Specialized Geriatric Centre, the Regional Geriatric Program of Northeastern Ontario, which is based Sudbury, ON. Her work advances quality improvement and integrated care for older adults.
Amanda Gardhouse, MD, FRCPC, is the geriatric medicine physician lead at North Simcoe Muskoka Specialized Geriatric Services, Barrie, ON, and community geriatrician with Couchiching Family Health Team, Orillia, ON.
Sean Goldhar, MD, CCFP (COE), is a family physician with a focus on care of the elderly clinical practice and medical education and affiliated with the Division of Geriatric Medicine, Queen's University, in Kingston, ON.
George Heckman, MD, FRCPC, is a clinician researcher affiliated with St. Joseph's Health Care London, and the Lawson Research Institute, in London, ON, and vice chair of the interRAI Instrument and Systems Development Committee.
Allison Hewitt, RN, works as a seniors' outreach nurse at Centretown Community Health Centre, in inner city Ottawa, ON and as a geriatric emergency management nurse at the Ottawa Hospital, also in Ottawa, ON.
Mark Lachmann, MD, FRCPC, is from Sinai Health, in Toronto, Ontario. Mark is a geriatric psychiatrist and co-medical director at Provincial Geriatrics Leadership Ontario, with a community team-based home visiting practice in East Toronto, ON.
Heather MacLeod, OT Reg. (Ont.), DSc, is director of programs and partnerships at Provincial Geriatrics Leadership Ontario and is based in Ottawa, ON.
Chantelle Mensink, MScN, PHC-NP, is a geriatric nurse practitioner with experience leading an interdisciplinary geriatric team in a primary care setting and works at the KW4 Integrated Care Team in Kitchener, ON.
Adam Morrison, MSc, CHE, is the senior director of public policy and partnerships at the Alzheimer Society of Ontario, based in Toronto, ON.
Mihaela Nicula, MD, FRCPC, is a community geriatrician and geriatric medicine lead in Brantford and Brant County and works at Brantford Community Healthcare and Grand River Community Health Centre in Brantford, ON.
Jagger Smith, MHA, leads specialist clinics, interprofessional outreach teams and integrated care models serving complex older adults in hospital, community and long-term care at Baycrest Hospital, in Toronto, ON.
Fran Wolfe, RN(EC), MScN, is a nurse practitioner who feels privileged to have learned from many older adults during her many years of practice at Baycrest Hospital in Toronto, ON.
Kevin J. Young, MD, Phd, FRCPC, is a geriatrician, the vice president medical affairs and chief of staff at Waypoint Centre for Mental Health Care in Penetanguishene, ON, and the co-medical director at Provincial Geriatrics Leadership Ontario, and is based in Penetanguishene, ON.
References
Aggarwal, R., S. Brar, M. Goodstadt, R. Devitt, S. Penny, M. Ramachandran et al. 2023. Using Comprehensive Geriatric Assessment in Identifying Care Goals and Referral Services in a Frailty Intervention Clinic. Canadian Geriatrics Journal 26(4): 530–7. doi:10.5770/cgj.26.683.
Alzheimer Society of Ontario. 2025, February. Dementia-Ready Ontario: 2025 Recommendations. Retrieved January 11, 2026. <https://alzheimer.ca/on/sites/on/files/documents/Dementia-Ready%20Ontario%20-%20Election%202025.pdf>.
de Levante Raphael, D. 2022. The Knowledge and Attitudes of Primary Care and the Barriers to Early Detection and Diagnosis of Alzheimer's Disease. Medicina 58(7): 906. doi:10.3390/medicina58070906.
Dimitriadou, I., A. Toska, S. Eloranta, S. Mört, N. Korsström, A. Lundberg et al. 2025. Comprehensive Geriatric Assessment: Addressing Unmet Healthcare Needs in Older Adults. Healthcare 13(21): 2715. doi:10.3390/healthcare13212715.
Heckman, G.A., S. Gimbel, C. Mensink, B. Kroetsch, A. Jones, A. Nasim et al. 2025. The Integrated Care Team: A Primary Care Based-Approach to Support Older Adults With Complex Health Needs. Healthcare Management Forum 38(3): 192–9. doi:10.1177/08404704241293051
Horgan, S., K. Kay and A. Morrison. 2020, August. Designing Integrated Care for Older Adults Living With Complex and Chronic Health Needs: A Scoping Review. Provincial Geriatrics Leadership Ontario. Retrieved January 11, 2026. <https://geriatricsontario.ca/wp-content/uploads/2020/11/PGLO-Scoping-Review-FINAL.pdf>.
Kay, K., S. A. Hawkins, A.M.B. Day, M. Briscoe, D. Daly and K. Wong. 2017, October 25. A Competency Framework for Interprofessional Comprehensive Geriatric Assessment. Provincial Geriatrics Leadership Ontario. Retrieved January 11, 2026. <https://geriatricsontario.ca/wp-content/uploads/2019/03/A-Competency-Framework.pdf>.
Lee, L., W.W. Weston and L.M. Hillier. 2018. Education to Improve Dementia Care: Impact of a Structured Clinical Reasoning Approach. Family Medicine 50(3): 195–203. doi:10.22454/FamMed.2018.221401.
Ministry of Health. 2025, January. Ontario's Primary Care Action Plan: Connecting Every Person in Ontario to Primary Care. Retrieved January 11, 2026. <https://www.ontario.ca/files/2025-01/moh-ontario-primary-care-action-plan-overview-2025-01-27.pdf>.
Molnar, F. and C.C. Frank. 2019. Optimizing Geriatric Care with the GERIATRIC 5Ms. Canadian Family Physician 65(1): 39. https://pmc.ncbi.nlm.nih.gov/articles/PMC6347324/.
Nalla, N. and S. Ehsan. 2025. Enhancing Comprehensive Geriatric Assessments in Ontario and Canada – Best Practices, Optimization, and the Role of Interprofessional Teams Seniors Care Network. Retrieved April 8, 2026. <https://fe1c8b0b-1f0b-4ee0-8fe1-153417952f4e.filesusr.com/ugd/d93231_aba8cc0c5e0d418688350c319f784e7d.pdf>.
Pham, A.N.Q., I. Akram, M.H. Tiwana and J. Smith. 2025. Trends in Access to Primary Care Among Canadian Older Adults Before, During, and Following the COVID-19 Public Health Emergency. Scientific Reports 15(1): 40629. doi:10.1038/s41598-025-24365-1.
Provincial Geriatrics Leadership Ontario (PGLO). 2026. Estimated Number of Older Adults Living With Frailty in Ontario. Retrieved April 6, 2026. <https://geriatricsontario.ca/resources/frailty-estimates-by-census-division-and-ontario-health-region/>.
Singh, S., A. Gray, S. Shepperd, D.J. Stott, G. Ellis, A. Hemsley et al. 2022. Is Comprehensive Geriatric Assessment Hospital at Home a Cost-Effective Alternative to Hospital Admission for Older People? Age and Ageing 51(1): afab220. doi:10.1093/ageing/afab220.
Warren, C., L. Mondor, S. Bronskill, M. Paterson, L. Plumptre and D. An. 2023. Characteristics and Utilization of Physician Specialist Services Among Older Adults With Dementia and Frailty in Ontario – 2023 Update, Applied Health Research Questions (AHRQ) # 2024 0800 263 001. Institute for Clinical Evaluative Sciences.
Weaver, L. 2021. The Collaboration Spectrum Revisited. Retrieved January 11, 2026. <https://www.tamarackcommunity.ca/hubfs/Resources/Publications/Collaboration%20Spectrum%20Revisited_Liz%20Weaver.pdf>.
Comments
Be the first to comment on this!
This article is for subscribers only. To view the entire article
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed